
Perioperative Cardiac Arrhythmias

– Dr. Nikhil Balankhe
Cardiac rhythm disturbances are one of the most misunderstood, frustrating and potentially devastating experiences for any anaesthetist inside the operation theatre. Though most of them are benign, there are quite a few arrhythmias which are nightmare for the anaesthetists. Almost 70.2 % patients subjected to general anaesthesia get these arrhythmias.
Pathogenesis of arrhythmias:-
- Injury to conduction system,
- Re-entry phenomenon,
- Automaticity,
- Mutations in the ion channels,
- Ectopic foci.
Causes – There are multiple reasons that contribute to the causation of these arrhythmias. They include – hypoxia, hypovolemia, hypokalaemia, hypomagnesemia, hypocalcemia, hypothermia, acidosis, light plane anaesthesia, cardiac ischemia, toxins, drugs, cardiac tamponade, tension pneumothorax, pulmonary thrombosis, and trauma.
Tracheal intubation is one of the most com¬mon cause of arrhythmias during induction as well as during the perioperative period, most often asso¬ciated with haemodynamic disturbances. Halothane or Enflurane produces arrhythmias, probably by a re-entrant mechanism. Regional anaesthesia (epidu¬ral anaesthesia) followed by central neuraxial block-ade may be associated with pharmacological sym¬pathectomy leading to parasympathetic dominance causing bradyarrhythmias. Abnormal blood gases such as hypercarbia, hypoxaemia or electrolyte imbalance like hypokalemia or hyperkalemia can produce arrhythmias either by producing re-entrant mechanism or by altering phase depolarization of conducting fi¬bers. Vagal stimulation due to trac¬tion on the peritoneum or direct pressure on the va¬gus nerve during carotid artery surgery may produce bradycardia or atrioventricular (AV) blocks, or even asystole. Dental surgery causes profound stimula¬tion of both sympathetic and parasympathetic ner¬vous stimuli.
The arrhythmias that are observed during perioperative period can be broadly divided into Bradyarrhythmias and Tachyarrhythmias.
Bradyarrhythmias can be of different types. They are:-
Sinus Bradyacardia – In these the Heart rate is less than 60/min.
The causes of sinus bradycardia are as follows:
- Drug effects – beta blockers, digitalis etc. . . .
- Acute myocardial ischemia/infarction
- Hypothermia
- Underlying hypothyroidism, cholestatic jaundice or raised intracranial pressure.
- Chronic degenerative change such as fibrosis of the atrium and sinus node.

Fig. 1 – SINUS BRADYCARDIA
Treatment- Asymptomatic bradycardia usually does not require treatment. In Symptomatic bradyarrhythmias if patient is haemodynamically compromised then atropine is the first line of treatment. It can be used in the dose of 0.5 to 1.0 mg (IV bolus), repeated every 3 to 5 minutes.
Heart block:
Heart blocks (AVHB) are broadly classified into three categories-
- First degree heart block
- Second degree heart block
- Complete heart block.
These may be transient or permanent.
Management: No treatment is required in first degree, 2nd degree and narrow complex 3° block except for eradication of toxic causes if any. Occasionally, permanent pacing is advocated for symp¬tomatic isolated AV block. While in broad complex blocks Temporary /Permanent Pac¬ing is indicated to maintain the normal hemodynamics.

Fig. 2 – First Degree Heart Block

Fig. 3 – Second Degree Heart Block
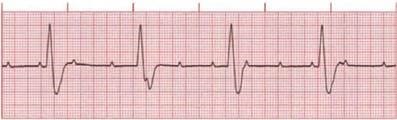
Fig. 4 – Complete Heart Block
Tachyarrhythmia –
These can be narrow QRS or wide QRS. Most wide complex (broad com¬plex) tachycardias are ventricular in origin.
Narrow QRS complex (QRS<0.12):
In these type of arrhythmias the QRS complex is less than 0.12 sec.
a. Sinus tachycardia: It is defined as an increase in the sinus rate of more than 100 beats/minute. Prolonged tachycardia for long duration can induce ischaemia in coro¬nary artery disease patients.
Causes: It includes Anaemia, Pain, Inadequate anaesthesia, Hypovolaemia, Fever, Hypercarbia, Thyrotoxicosis/ thyroid crisis and Cardiac failure.

Fig. 5 – Sinus Tachycardia
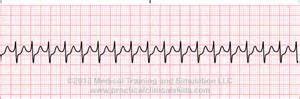
Fig. 6 – Supraventricular Tachycardia
Treatment: Precipitating factors must be identified and corrected. Drug therapy is required in patients with ischemic heart disease who develop ST segment changes to prevent further myocar¬dial ischemia. Beta-blockers such as esmolol is preferred drug. It has half-life of 10 min with bolus dose of 500 mcg/kg over 1 min, followed by an infusion of 50-300 mcg/kg/min. If continuous use is required, it may be replaced by longer lasting cardio se¬lective drugs such as metoprolol in the dose of 5 to 10 mg given slowly intravenously at 5 min interval to a total dose of 15 mg.
b. Atrial premature beat: It represents 10% of all intraoperative arrhythmias. Treatment is not nor¬mally required unless the ectopic beats provoke more sig¬nificant arrhythmias, where β blockade may be effective.
c. Atrial tachycardia: These arrhythmias are found in 6% of patients undergoing non cardiac surgery. It is non-paroxysmal, narrow QRS rhythm with retrograde P waves with rate less than 70 beats/min. If faster usually less than 130 beats/min, it is termed as accel¬erated AV junctional rhythm. These arrhythmias can lead to fall in blood pressure up to 15% in patients without car¬diac disease and up to 30% in diseased heart.
Treatment – Usually no treatment is required; carotid sinus massage and verapamil are often helpful in symptomatic patients. Intravenous ad-enosine in 6 to 12 mg doses is another alternative.
d. Atrial flutter: This is a rhythm disturbance that is usually associated with organic or ischaemic heart disease. The atrial rate varies between 280 and 350 /min but is usually around 300/ min.

Fig. 7 – Atrial Flutter
Treatment: Treatment of an acute paroxysm is electrical cardio version. Prophylaxis is achieved with class Ia, Ic or III drugs in diseased heart patients.
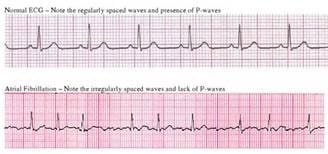
Fig. 8 – Atrial Flutter
Treatment – The precipitating or provoking agents should be removed or treated first. Intravenous beta-blockers or calcium channel blockers produce rapid control of rate, regardless of the level of sympathetic tone. However beta-blockers are preferred over calcium channel blocker (CCB) during intraoperative period due to shorter duration of action and lesser negative inotropic effects. In haemodynamically-compromised patients, DC cardioversion is the most effective method of converting AF to sinus rhythm. Chronic AF is often found in patients with rheumatic heart disease undergoing cardiac surgery and may have atrial thrombi; therefore, any attempt to restore sinus rhythm by DC cardio version may be associated with increased risk of systemic or pulmonary embolisation. Successful cardio version is relatively rare in chronic AF. The control of ventricular rate is the preferred approach in these cases. The most useful drug for this purpose is digoxin. The patients with chronic AF undergoing non cardiac surgery should be evaluated for the presence of atrial clot by echocardiogram prior to surgery. In the presence of atrial clot, control of ventricular response rate with appropriate medication is instituted during perioperative period, if necessary.
a. Lidocaine with an initial bolus dose of 1.5 mg/kg followed by infusion of 1 to 4 mg/min can be given. Other drugs from class I, II or III are used to treat these types of arrhythmias.
b. Ventricular tachycardia
This is defined as three or more consecutive ventricular beats occurring at a rate of 120 bpm or more. It may be poten¬tially life threatening.

Fig. 9 – Ventricular Tachycardia
Ventricular Tachycardia Treatment may be urgent depending on the hemodynamic situation. If the cardiac output and the blood pressure are very depressed, emergency DC cardio version must be considered. On the other hand, if the blood pressure and cardiac output are well maintained, intravenous therapy with class I a drug is usually advised. First-line drug treatment consists of lidocaine (50-100 mg i.v. over 5 min) followed by a lidocaine infusion (2-4 mg/min i.v.). DC-cardio version may be necessary if medical therapy is unsuccessful. The administration of multiple anti arrhythmic drugs should be avoided. Patients with recurrent episodes or unresponsive to lidocaine, may require therapy with procainamide (10-15 mg/ kg loading dose followed by an infusion of 2 to 6 mg / min ) or bretylium (5 to 10 mg / min over 2 to 5 min then infusion of 1-2 mg / min ) or amiodarone in the dose of 150 mg IV over 10 minutes followed by an infusion of 1 mg / min for 6 hours and 0.5 mg / min thereafter. IV amiodarone has been shown to be as effective as bretylium with added advantage of less hypotension as compared to IV bretylium.
C.Ventricular fibrillation(VF) It is very rapid and irregular ventricular activation with no mechanical effect. It is usually intiated from an ischemic myocardium or an aberrant foci (especially in acute preoperative myocardial infarction), ventricular tachycardia or torsades de pointes. On ECG, there are no defined QRS complexes, shows shapeless rapid oscillations and on pulse oximetry, there is acute fall in SpO 2 because of low or no cardiac output. Causes include myocardial ischemia, hypoxemia, electrolyte imbalance and drug effects.
Treatment: Cardiopulmonary resuscitation must be performed as rapidly as possible. Asynchronous external defibrillation should be performed using 200-360J. A precordial thump is occasionally effective in terminating VF, but should be attempted only if a defibrillator is not available immediately. Intravenous bretyium 5-10 mg.kg -1 over 5 min can be useful on some occasion. Supporting pharmacological therapy such as lidocaine, amiodarone and procainamide are used only to prevent recurrence of VF.
