
Anaemia and Anaesthesia Interaction
– Dr. Subhada Deshmukh
Professor, Dept. of Medicine,
NKPSIMS
Professor, Dept. of Medicine,
NKPSIMS
Introduction
The World Health Organization defines anemia as hemoglobin <13 g/dL in men and <12 g/dL in non-pregnant women. In pregnancy, anaemia is defined as a Hb concentration of 11gm% in first and third trimester and Hb of <10.5 g/dL in second trimester (to adjust for increase in plasma volume).
Prevalence of anaemia in India – The prevalence of anaemia in India is high and some figures quoted are as follows –
- Lancet/ The Indian Express – The incidence of anaemia is 55.3% among women in reproductive age group, 53.2% in non-pregnant, non-lactating women and 69.5% in children under 5 years of age.
- Int J Biomed Res 2012; 3(4):2422-28 – In healthy young males and females in North India, 53.2% males and 70.1% females were found to be anaemic.
- Journal of Clinical and Diagnostic Research 2011 – Prevalence of anaemia among apparently healthy young males and females from rural Punjab is about 89% in both.
- National Family Health Survey – 2005-2006 – Anaemia is prevalent in 56% adolescent girls and 30% adolescent boys..
Anaemia should be viewed as a serious and treatable medical condition, rather than simply an abnormal laboratory value. Depending on procedures and definition of anaemia, upto 75% of patients for elective surgery may be anaemic and upto 90% patients may have anaemia in the postoperative period. The overall prevalence of anaemia in general population increases with age and so many elderly (≥ 65 years) patients presenting for surgery may be anaemic. These patients often present for orthopaedic surgery like fixation of fractures and joint replacement. Orthopaedic procedures are associated with considerable blood loss in the intraoperative period and postoperative periods (in drains).
Three randomized trials in adults and children demonstrated that lower Hb thresholds were well-tolerated in critically ill patients and cardiac surgical patients. The physiological premise that acute hemodilution optimized blood rheology and favoured perfusion led to clinical approaches that further reduced red cell mass in a number of clinical settings. The collective impact of these influences promoted a tolerance for acute and chronic anemia.
But a number of clinical studies have shown that anaemia is associated with morbidity and mortality in the perioperative period. Anemia is a potent multiplier of morbidity and mortality risk, including in the perioperative setting. In a retrospective study of 1958 Jehovah’s Witness patients undergoing non-cardiac surgery, a preoperative Hb concentration of ≤10 g dl was associated with a significant increase in perioperative mortality. This increase was significantly more pronounced in patients with cardiovascular disease (CVD) than in patients without known CVD. A decrease in Hb of ≤2 g/ dl in the absence of CVD was not associated with an increased risk of postoperative death. The risk of death was highest in patients with CVD along with a ≥4 g/ dl or greater decline in Hb. In a subsequent analysis, for all patients, postoperative Hb levels ≥7 g/ dl were associated with some morbidity but no mortality; but for every 1 g /dl decrement below 7 g dl21, mortality risk increased by a factor of 1.5.
Chronic anaemia is a risk factor for acute intraoperative anaemia. It appears that in patients without cardiovascular disease, the tolerance for postoperative anaemia is high. But in patients with cardiovascular disease, the tolerance for anaemia is lower and these patients benefit particularly from anaemia management.
Physiological response to anaemia –
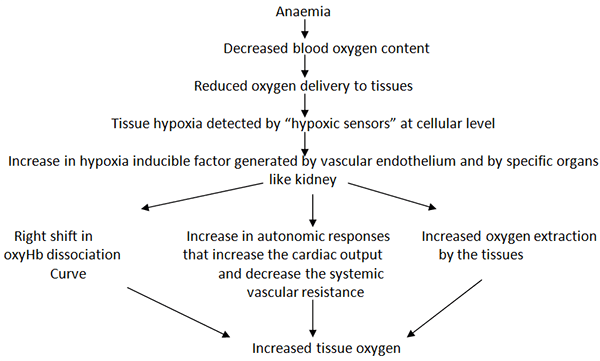
Any factor that interferes with these mechanisms in general and specifically with the increase in cardiac output (β blockade) or local organ specific vasodilatation may disrupt tissue oxygen delivery during acute anaemia (normovolaemic). Although myocardial oxygen consumption increases due to increased heart rate and contractility, an overall reduction in metabolic requirements in other tissues helps to balance oxygen demand and supply. Hence if this situation changes due to any cause like fever, thyrotoxicosis etc., anaemia will cause tissue hypoxia at Hb levels which otherwise would have been tolerated by the patient. Oxygen extraction is an important determinant of adequacy of tissue oxygenation. Normal mixed venous partial pressure of oxygen (PvO2) is 35-45 mm Hg and SvO2 is 72-75%. In chronic anaemia, cardiac output increase maintains a constant arterial to venous oxygen difference and the oxygen extraction ratio is normal (25%). But when there is an acute rise in oxygen demand, the oxygen extraction increases and SvO2 falls along with further possible increase in cardiac output. Acute cardiac failure may result due to excessive strain on the myocardium.
Risk of preoperative anaemia –
The key consequence of acute anaemia is reduced blood oxygen content leading to reduced oxygen delivery to the tissues and hence tissue hypoxia. The exact mechanisms of organ dysfunction and mortality have not been clearly defined. However, experimental studies have demonstrated that acute anaemia can result in reduction in tissue partial pressure of oxygen which supports the hypothesis that tissue hypoxia could be a significant mechanism of anaemia-induced organ injury and mortality. During anaemia, brain and heart (organs critically important for survival) receive preferential oxygen delivery and hence brain oxygen delivery can be maintained at low levels of Hb (approx 3.5 to 4 gm/dL) while kidney, liver and lungs suffer hypoxia at higher Hb levels ( 6 to 7 gm/dL).
Hb thresholds for individual patients for organ injury and mortality are not known. Some tolerate Hb levels near 7 gm/dL but it is also seen that mortality and neurological injury is increased following cardiopulmonary bypass at this Hb. Optimal Hb may be approx 10 gm/dL for patients suffering from neurotrauma or acute coronary syndrome.
In surgical patients with low admission and discharge Hb levels, the clinical evidence of impaired oxygen delivery can be seen as –
- Increased postoperative mortality
- Increased major cardiovascular events
- Increased length of hospital stay
- Increased readmission rates
- Reduced quality of life
- Impaired functional recovery
- Increased incidence of wound infection and delayed wound healing.
In addition there could be risk of therapies that impair cardiovascular responses to anaemia, particularly acute β blockade. The POISE (PeriOperative ISchaemia Evaluation) trial emphasized the paradoxical potential for cerebral injury despite myocardial protection in acutely β-blocked (Metoprolol 200 mg given 2 hours before surgery) patients undergoing non-cardiac surgery. The risk of stroke was increased by about 2-fold in β-blocked patients who experienced intraoperative bleeding. A subsequent retrospective analysis also demonstrated a paradoxical increase in acute cardiac events in β-blocked patients who experienced fall in Hb levels. Another study identified an increase in preoperative MI in β-blocked who experienced blood loss and Hb levels < 10 gm/dL. Thus treatment with β-blockers may accentuate the risk of organ ischaemia (brain, heart) in the setting of acute blood loss. The mechanism involved may be global impairment of cardiac output response (β1-blockade) and impaired microvascular dilatation (β2-blockade).
Postoperative Anaemia –
Postoperatively, anaemia resembles anaemia of chronic disease and is probably related to the effects of inflammatory mediators released during and after surgery on the production and survival of RBCs. Proinflammatory cytokines, such as tumour necrosis factor released during
surgery and trauma invoke a response characterized by decreased iron uptake from the gastrointestinal tract and iron sequestration in macrophages, along with a diminished erythroid response to erythropoietin and decreased erythropoietin production.
Other causes of postoperative anaemia include pre-existing preoperative anaemia and traumatic and surgical blood loss. Also, there is an element of haemodilution occurring as a result of fluid replacement before, during, and after surgery. Normovolaemic haemodilution is well tolerated due to compensatory mechanisms that maintain an adequate myocardial and peripheral tissue oxygenation. On the other hand, hypovolaemic anaemia must be avoided, as the cardiovascular compensatory mechanisms required to maintain oxygen transport in the setting of anaemia are severely compromised.
Risks of Blood Transfusion –
Preoperative autologous donation is generally not cost-effective but may be of value in selected patient populations, such as in patients previously alloimmunized with erythrocyte antibodies. Acute normovolemic hemodilution causes blood losses during surgery to be diluted, thus reducing actual total blood losses. However, evidence on efficacy of acute normovolemic hemodilution is mixed. Reasons for low acceptance include lack of standardized protocols, variations in the target hemoglobin, types of fluids used, heterogeneity in surgical blood losses by procedure, and patient selection criteria. Acute normovolemic hemodilution is most effective in procedures associated with large blood loss. Because some large blood loss surgical procedures may not result in significant blood loss, benefit of acute normovolemic hemodilution may not be realized.The risk of monitored acute normovolemic hemodilution is extremely low and this still favors acute normovolemic hemodilution.
Allogenic blood transfusion continues to be the most frequently used means of treating acute severe intraoperative blood loss. Goal of red cell transfusion is to restore adequate tissue oxygen delivery.
Risks associated with allogenic transfusion are –
- Febrile non-haemolytic transfusion reaction
- Allergic reactions – Urticarial rash to anaphylaxis
- Transfusion related acute lung injury
- Transfusion related acute circulatory overload
- Immunomodulation (mild to severe)
- Death
Multiple studies have shown an association of allogenic blood transfusion with postop infections, prolonged hospital stay, increased morbidity and mortality, increased risk of thrombotic events and decreased disease-free survival in cancer patients.
An interesting factor in the relation between transfusion and outcomes is the shelf life of the blood being transfused. Currently storage of blood for a maximum of 42 days is allowed, but a recent study of patients who received red blood cell transfusions during cardiac surgery found that those who received “older blood” (stored for > 14 days) had significantly higher rates of sepsis, prolonged intubation, renal failure, in-hospital mortality, and 1-year mortality compared with those who received “newer blood” (stored for ≤ 14 days).
These different outcomes are attributed to the so-called storage defect: as blood gets older, it loses components such as 2,3-DPG and adenosine disphosphate, its red cells lose deformability, and it undergoes buildup of cytokines and free hemoglobin.
Considering the risks of both anaemia and allogenic blood transfusion, diagnosis and treatment of acute or chronic anaemia prior to elective surgery may reduce morbidity and mortality associated with both.
A multidisciplinary panel of physicians was convened by the Network for Advancement of Transfusion Alternatives (NATA) with the aim of developing practice guidelines for the detection, evaluation, and management of preoperative anaemia in elective orthopaedic surgery. NATA algorithm on approach to the diagnosis and treatment of anaemic patients is given below. Recommendations of NATA are as follows –
- Recommendation 1 – Detection of Anaemia – NATA recommends that elective surgical patients have Hb level determination as close to 28 days before the scheduled surgical procedure as possible (Grade 1C).
- Recommendation 2 – NATA suggests that the patient’s target Hb before elective surgery be within the normal range according to WHO criteria (≥12gm/dL in females and ≥13 gm/dL in males.
- Recommendation 3 – NATA recommends that lab testing be performed to further evaluate anaemia for nutritional deficiencies, chronic renal insufficiency and/or chronic inflammatory disease (Grade 1C).
- Recommendation 4 – NATA recommends that nutritional deficiencies be treated (Grade 1C). An expert panel reviewed the role of IV iron in the management of perioperative anaemia and concluded that patients with preoperative anaemia due to iron deficiency or chronic disease should receive preoperative treatment with oral or IV iron, depending the time scale before surgery, tolerance of oral iron,and iron status.
- Recommendation 5 – NATA suggests that ESA be used for anaemic patients in whom nutritional deficiencies have been ruled out, corrected or both (Grade 2A).
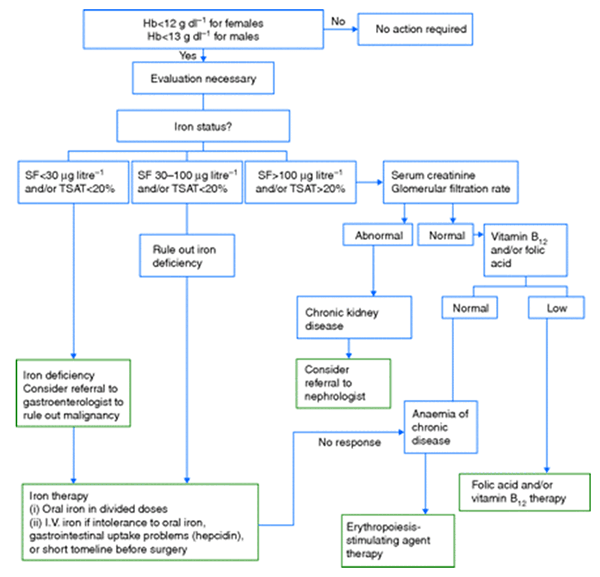
Proposed algorithm for the detection, evaluation, and management of preoperative anaemia. SF, serum ferritin; TSAT, transferrin saturation.
NATA also advises that the diagnosis of an unexpected anaemia in patients undergoing elective surgery in which a significant amount of blood loss is expected should be considered as an indication for rescheduling the surgery until evaluation is complete.
Few points to remember about the treatment outlined above are as follows –
- The major clinical difference between oral and IV iron therapy is the speed of Hb increase (30-40 days vs 7-14 days) and replenishment of iron stores. Maximal oral uptake is 5 to 10 mg/day.
- With IV iron therapy, effect on Hb levels starts occurring in 1 wk & maximum effect is achieved in 2 wks.
- Use of Erythrocyte Stimulating Agents – e.g, recombinant human erythropoietin – ESAs have been studied in orthopaedic and cardiac surgeries. In these patients, ESAs have been shown to increase Hb levels, reduce allogenic transfusions, increase aerobic capacity and improve quality of life. Adverse effects of these agents are increased thrombotic events and cancer progression. So, a graded approach is recommended: ESAs are recommended for unresponsive iron-deficiency anaemia in which a component of anaemia of chronic disease is suspected. Aim of therapy is to increase Hb levels to 10-12 gm/dL in major elective surgeries associated with significant risk of blood loss and requiring blood transfusion.
- ESAs should not be administered to iron-deficient patients unless iron supplementation is provided adequately simultaneously as some studies suggest that ESA-driven erythropoiesis in an iron-deficient individual may lead to increase in thrombotic event.
- Since use of ESA is associated with thrombotic events, use of thromboprophylaxis is necessary.
Choice of Anaesthesia –
In anaemic patients who have to be taken up for surgery, the choice of the actual anaesthetic technique employed will depend on the severity and type of anaemia, extent of physiological compensation, concomitant medical conditions, type of surgical procedure to be done and the anticipated blood loss. The main anaesthetic considerations in chronic anaemia are to minimize factors interfering with oxygen delivery and prevent any increase in oxygen consumption.
The principles to be adhered to while giving anaesthesia, whether GA or Regional Anaesthesia can be listed as follows –
- Avoidance of hypoxia –
- Preoxygenation with 100% oxygen.
- Oxygen supplementation in the intra and postoperative periods.
- Maintenance of clear and patent airway. This prevents a fall in FiO2 due to airway obstruction.
- Spontaneous ventilation be used only for short procedures for fear of hypoventilation.
- Aggressive treatment of conditions that increase oxygen demand like fever, shivering and of acute blood losses leading to an acute drop of Hb below 7 gm/dL.
- Blunting the sympathetic response to laryngoscopy and intubation during GA.
- Minimizing drug-induced decreases in cardiac output –
- Intravenous induction of anaesthesia should be slowly titrated to prevent precipitous fall in cardiac output.
- Careful positioning of patient to minimize position associated volume shifts.
- Mild tachycardia and wide pulse pressure may be physiological and should not be confused with light anaesthesia.
- Factors leading to leftward shift of Oxy-Hb dissociation curve (ODC) –
- Avoidance of hyperventilation as it causes hypocapnia as well as respiratory alkalosis. Both cause a left shift in ODC.
- Avoidance of hypothermia by the use of warming blankets and use of warmed IV fluids, blood and also irrigation fluids.
- Monitoring – Should be aimed at assessing the adequacy of perfusion and oxygenation of vital organs. Monitoring should include ECG, NIBP, EtCO2, Pulse oximetry, temperature monitoring, Urine output measurement. CVP, Invasive arterial pressure measurement, estimation of mixed venous O2 (PvO2) and ABG analysis can be used when major losses are anticipated.
Serial estimation of Hb and Hct values give an idea about ongoing losses. - Regional anaesthesia is preferred for peripheral limb surgery as it is associated with reduced blood loss.
- Central Neuraxial Blockade – Can be used judiciously. Problems could be hypotension, haemodilution and subsequent heart failure or pulmonary edema on the return of vascular tone. It is advisable to use vasoconstrictors to sustain blood pressure rather than give high volumes of IV fluids.
Patient Blood Management
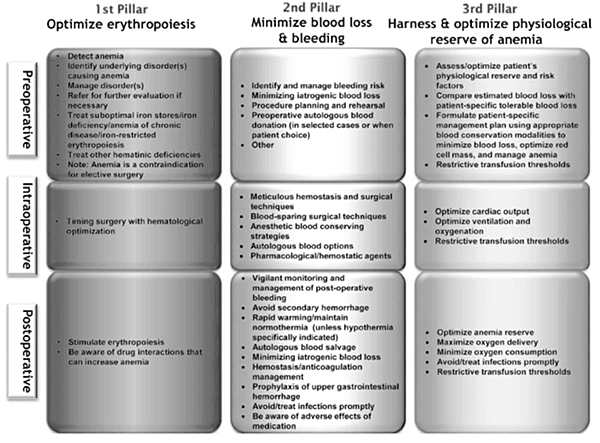
Patient Blood Management (PBM) employs a patient-specific peri-operative multi-disciplinary, multimodal team approach to optimize, conserve and manage patients’ own blood. PBM aims to identify patients at risk of anaemia and provide a managed plan aimed at reducing or even eliminating the need for allogeneic transfusion with an acceptable risk of anaemia and, as a consequence, at improving postoperative outcome. Evaluating the peri-operative period of elective surgical interventions, 98% of all cases of red blood cell transfusions can be predicted if 3 parameters are analysed. These parameters are the pre-operative haemoglobin, blood loss and individual transfusion trigger. Therefore, PBM is fundamentally based on 3 pillars:
- Optimization of the (pre-operative) red cell count.
- Reduction of diagnostic, interventional and peri-operative surgical blood loss.
- Optimizing individual tolerance of anaemia and accurate (restrictive) indication for blood transfusion.
Patient blood management has recently been recognized by the World Health Organization (World Health AllianceResolution A63.R12) as a means to “promote the availability of transfusion alternatives
References –
- Hare G, Baker JE, Pavenski K. Assessment and treatment of Preoperative anaemia.
Can J Anesth 2011, 58:569-81 - Singh S, Gudzenko V, Fink MP. Pathophysiology of perioperative anemia.
Best Practice & Research Clinical Anaesthesiology2016; 26 : 431–439 - Beris P, Munoz M, Garcia-Erce JA, ThomasD, Maniatis A, Vanderlinden P. Perioperative anemia management: Consensus statement on the role of intravenous iron.
Br J Anaesth 2008; 100(5):599-604 - Sear JW, Giles JW, Howard-Alpe G, Foex P. What does the POISE study tell us?
Br J Anaesth 2008;101(2):135-8 - Grewal A. Anaemia and Pregnancy: Anaesthetic Implications.
Indian J Anaesth 2010;54(5):380-6 - Koch CG, Li L, Sessler DI et al. Duration of red cell storage and complications after cardiac surgery. N Eng J Med 2008;358:380-6.
- Goodnough LT, Shander A. Patient Blood Management. Anesthesiology 2012; 116:1367-76
- Goodnough LT, Maniatis A, Earnshaw P, Benoni G, Beris P, Bisbe E et al. Detection, evaluation and management of preoperative anaemia in the elective orthopaedic surgical patient: NATA guidelines. Br J Anaesth 2011; 106 (1): 13–22
- Gombotz H. Preoperative anaemia and patient blood management.
EACTA 2012 | Abstracts | Invited speakers
