
CANCER PAIN MANAGEMENT

– Dr. Anjali Kolhe
M.D. ,F.U.I.C.C.(PAIN)
M.D. ,F.U.I.C.C.(PAIN)
CANCER PAIN MANAGEMENT
Cancer is considered as dreaded Disease for the fear of ‘pain and death’ associated
with it. Approximately 9 million new cases are diagnosed every year world-wide.
In developing countries the majority cancer patients present with advanced disease
and for such patients the only realistic treatment options are pain management and
palliative care.
The under- treatment of chronic cancer pain persists despite decades of efforts
to provide clinicians with information about analgesics and pain relieving techniques
for various reasons.
The important Cancer Pain Statistics are as follows :
- WHO estimates every year, 3.5 million people worldwide & Half a million
people in India suffer from cancer pain. - Pain is experienced by 20-50% patients when diagnosed or undergoing tratment
and 55-85% of patients with terminal cancer, with Overall average of nearly
75%. - Foley et al (1979) in their study found that Pain due to cancer in 78% and
Pain associated with cancer therapy 19% patients and 3% patients suffered from
Pain unrelated to cancer or therapy - Severity of pain – Moderate to severe pain experienced by 40-50% patients
amongst the advanced disease and 20-50% patients when diagnosed or undergoing
treatment. - Etiology of pain – Most have 2 or more types of etiologies of pain
- Treatment of pain- 70 – 90% patients can be controlled with analgesics &
adjuvants as per WHO analgesic ladder. And 10 – 30% of pain patients, require
interventional pain management.
WHY SO MUCH PAIN IN CANCER?
Cancer pain is multifactorial and caused mainly by tumor itself or secondary
to various cancer treatments (saunders C and Baines M 1983)
The common cancer pain syndromes resulting from above etiologies are:
- Pain syndromes related to direct tumor involvement:
- This will be secondary to progression of disease and infiltration of
structures in the body like- Soft tissue infiltration
- Infiltration of plexus or nerve roots or peripheral nerves
- Infiltration of bone
- Infiltration of base of skull or cranial nerve
- Pain due to bone involvement
- Base of skull syndrome
- Orbital syndrome
- Parasellar pain syndrome
- Sphenoid sinus syndrome
- Middle cranial fossa syndrome
- Clivus syndrome
- Jugular foramen syndrome
- Vertebral syndrome
- Atlantoaxial syndrome
- L1 Syndrome
- Pain due to neural involvement
- Peripheral nerve syndrome
- Painful polyneuropathy
- Brachial or lumbosacral plexopathy
- Leptomeningeal metastatases
- Epidural cord compression
- This will be secondary to progression of disease and infiltration of
- Syndromes related to cancer therapy
- Post Operative pain syndromes- e. g.
- post-thoracotomy,post mastectomy pain syndrome
- Post radical neck dissection pain syndrome,
- post amputation Pain syndrome
- Post-chemotherapy Pain Syndrome-Painful polyneuropathy painful
aseptic necrosis of femoral or humeral head, steroid pseudo rheumatism,
oral mucosistis. - Post radiation pain syndromes
- Radiation Fibrosis of brachial or lumbosacral plexuses
- Radiation Myelopathy
- Radiation induced secondary neoplasm
- mucositis
- Post Operative pain syndromes- e. g.
- Syndromes unrelated to Cancer
- Myofascial pains
- Herpes zoster
- Backache
- arthralgia
- headache
- bed sores
Management of Cancer Pain
The successful management of cancer patient with pain depends on the
- The ability of the clinician to assess initial problem
- Identify and evaluate the pain syndromes
- Formulate a plan for continuing care that is responsible to the revolving
goals and needs of the patient and patient’s family
Assessment of cancer pain:
Careful and comprehensive assessment of cancer pain is essential in finding
the best treatment for the pain. Initial assessment of pain should focus on
identifying the cause of pain and its management plan.
It includes comprehensive clinical history and examination of the patients as
follows:
- Details of Primary disease & it’s treatment.
- Characterize Pain –Onset, site, type, severity and duration, aggravating
and relieving factors. - Psychological, psychosocial assessment of the patients.
- General, Neurological examination.
- Specify various pain syndromes in cancer.
- Appropriate Lab., electro diagnostic & radiographic procedures
Neurophysiologic testing – EMG etc. - Measurement with different pain scales.
Pain Scales – Visual analog and 0 to 10 point numeric scales are used to measure pain. A process that allows frequent reassessment and therefore adequate treatment. If the patient understands the scale and is capable of answering and if end points and adjective descriptors are carefully selected, each of these instruments can be valid and reliable. Some of the scales to measure pain are as follows:

Approaches to pain management
After evaluation and assessment of the cancer pain patients the various approaches to pain management are as follows:
| Psychological Approach | Understanding, companionship Feeling of not being given up. |
| Modification of pathologic process | Radiation therapy Hormone Therapy Chemotherapy Surgery |
| Drugs | Analgesics Antidepressants Anxiolytics Neuroleptics |
| Interventional pain management | Augmentative Neurolytics- RF ablation, Cryo etc. Neurosurgery |
| Modification of daily activities | Rest, Cervical collar or ortho. Sx, Corset splints |
Primary anticancer treatment:
Antineoplastic therapies are used when pain is due to neoplasm
- Radiation therapy: gives adequate analgesic & pain is a common primary
indication for radiotherapy - Chemotherapy:
- Toxicity of drugs should be considered
- Unpredictable pain relief.
- Advised to complete cycles before major interventions,
- Hormone treatment to be considered for breast, prostate etc.
- Surgery: Vertebral body resection for epidural, spinal cord compression,
Surgery for bony fractures, Intestinal obstruction etc.
Symptomatic cancer pain management
Pharmacotherapy of cancer pain
Pharmacotherapy plays a very vital role in the management of cancer pain, as
almost 80 – 90% of the pain can be reasonably controlled using different
analgesics along with the adjuvants.
Opioid based therapy is mainstay in cancer pain Management
Three main groups of pharmacotherapy are
- Nonopoid analgesics
- Opioid analgesics
- Adjuvant drugs
A simple, well-validated, and effective method for assuring the rational titration of therapy for cancer pain has been devised by WHO. It has been shown to be effective in relieving pain for approximately 90 percent of patients with cancer and over 75 percent of cancer patients who are terminally ill. The World Health Organization (WHO) in 1986, established a stepladder approach for treatment of patients with cancer pain, which was later on modified in 2000 to include interventional pain management.
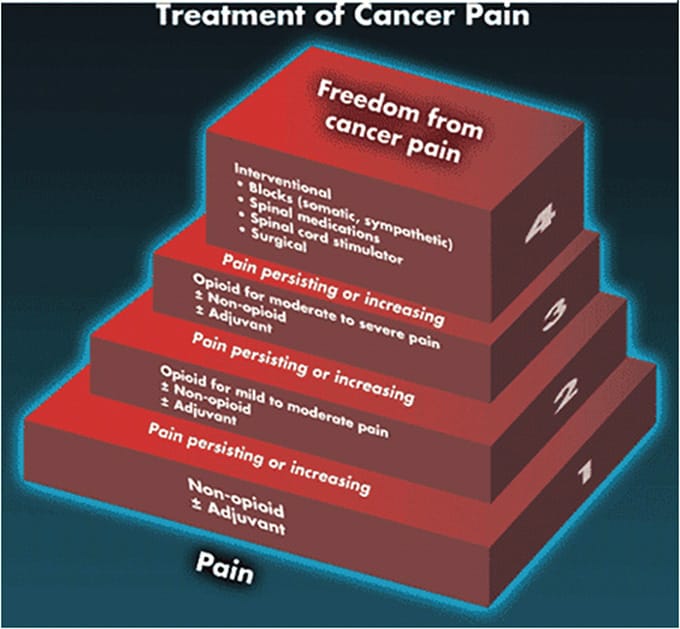
Modified “analgesic ladder” for cancer pain, including interventional management.
Adapted from World Health Organization. World Health Organ Tech Rep Ser. 1990; 804:1-73; Miguel R. Cancer Control. 2000; 7:149-156 and Krames E. Med Clin North Am. 1999; 83:787-808.
The seven essential concepts in the WHO approach to drug therapy of cancer pain are:
- By the mouth.
- By the clock.
- By the ladder.
- For the individual.
- With attention to detail.
- Use adjuvant drugs
- Monitored treatment (to maximise benefits and minimise adverse effects)
The first step in this ladder is the use of acetaminophen, or other NSAIDs for mild to moderate pain. Adjuvant drugs to enhance analgesic efficacy, or to treat concurrent symptoms that exacerbate pain may be used at any step.
When pain persists or increases an opioid such as codeine or hydrocodone should be added (not substituted) to the NSAID. Opioids at this step are often administered in fixed dose combinations with acetaminophen because this combination provides additive analgesia.
Pain that is persistent, or moderate to severe, should be treated by using more potent opioid or using higher dosages as shown in the third step. At this step separate dosage of opioid and nonopioid analgesic should be used to avoid the overdoses of acetaminophen or NSAID. Opioids like morphine, hydromorphone, methadone or fentanyl are used in this step.
A] NSAIDs, COX-2 Inhibitors, ASA, and Acetaminophen
An NSAID alone may be effective for mild cancer pain. It acts centrally by inhibiting the COX-2 production and thereby reducing the prostaglandin synthesis.
Relieves somatic / musculoskeletal / integumental pain / pain of bone metastases .They have Ceiling analgesics effect, a limiting factor They have Opioid dose sparing effect. Most widely used Analgesics are Ketorolac, Diclofenac, Ketoprofen, Ibuprofen.
Newer COX-2 Specific Inhibitors selectively inhibit only this enzyme, thus maintaining an anti-inflammatory response with low risk of side effects that occur with nonselective inhibitors. Recently, however, COX-2 inhibitors have received attention because of an increased incidence of stroke and myocardial infarction when used in high doses. Rofecoxib & Valdecoxib withdrawn recently. Parecoxib, Etorocoxib approved for short term treatment of moderate to severe pain.
Acetaminophen-
Useful in management of mild pain Proven analgesic with central mechanism of action. Inhibits NMDA mediated nitric oxide synthesis Proven efficacy in clinical settings involving central sensitization
B ] Opiods:
Mainstay of Pharmacotherapy in cancer pain Management for treatment of moderate to severe pain.
Opioid is any compound that binds to an opioid receptor and with morphine like properties
Three Schemes are used to classify opioids.
- Based on intrinsic action at the receptor site.
- Partial Agonist – Buprenorphine
- Agonist – e.g. Morphine,Codeine, Methadone, fentanyl
- Agonist – Antagonist – butorphanol, nalbupine, pentazocine,
- Antagonist – naloxone, naltrexone, Cholecytokinins.
- Based on affinity for opioid receptors
- Weak – Codeine, Propoxyphene
- Strong –Morphine, Fentanyl, Buprenorphine,Morphin etc
- Based on how opioid are derived
- Naturally occurring -morphine, Codeine
- Semisynthetic
- Synthetic
( Morphine, Codeine obtained from Phenanthrene alkaloids of opium)
Different routes for administration of Opioid Analgesics are used.
They are
Intravenous infusion for immediate relief in acute pain. Also used as Continuous infusions with PCA pumps, Infusion pumps,Mechanoelastic pumps e.g.Fentanyl 0.5-1 µgm/kg/hr Tramadol 30-40 mg/24 hrs.
Other routes of administration of Opioid Analgesics
Subcutaneous, Epidermal, Intrathecal, Intraventricular, Rectal, Sublingual,
Submucosal
Morphine: It is a gold Standard against which new drugs are measured. It has no pharmacological ceiling effect. Initial oral dose 20 – 30 mg 4-6 hourly, may vary 1000 fold. Controlled release – MS Contin 15,30,60 mg Tabs, immediate release 10, 30mg Tab, solution 20 mg / 5ml, Suppository, sublingual preparations. High 1st pass metabolism, bioavailability 25%. Adverse effects- constipation, respiratory depression, hypotension, Tolerance, dependence on chronic use.
Fentanyl: It is a Synthetic phenyl piperidine derivative. It has High potency and lipophilicity. It is 75-100 times more potent than morphine. Is Short acting 40-60 min. with 100 mg dose. Different preaparation available – Transdermal (Patches),Parenteral, Transmucosal.
Transdermal Therapeutic system Fentanyl (TTS-Fentanyl): Protective liner + Four layers, a drug reservoir, rate control layer etc. Amount of fentanyl released – 25 µgm/hr/10cm2. Concentration gradient between reservoir & concentration in skin drives the drug. Lag time of 2 hours for clinically useful systemic levels.72 hrs. release. Costlier Transdermal Fentanyl Provides continuous administration of highly potent analgesic.
Codeine: It is used in mild to moderate pain. Has low affinity for receptors; demethylation to morphine contributes to analgesic action.
- Oral dose 30-60 mg 4-6 hourly.
- Adverse effects constipation, drowsiness, respiratory depression.
- Available in combination with acetaminofen, NSAID.
Pentazocine – k agonist, μ antagonist, partial agonist
– Oral dose 50-100 mg 4-6 hourly
– Adverse effects ↑ se H.R., B.P. (Sympathetic stimulation), Psychotomimetic effects, anxiety, depression; useful in acute pain.
Buprenorphine – 25-50 times more potent than morphine. Slower onset, longer duration of action. It has Ceiling effect Causes Postural Hypotension. Used by Parenteral, sublingual, spinal administration.
Tramadol – Weak μ agonist, inhibits uptake of NE, 5-HT. Oral dose 50-100 mg 6 hourly. Adverse effect are drowsiness, dizziness, dry mouth, drug induced Seizures.
Methadone – methadone hydrochlorides, a Synthetic opioid Oral, rectal, parenteral preparations available. It has excellent oral, rectal absorption, High potency, High lipid solubility, Low cost, long duration.
Naloxone – Used as Opioid antidote. Is used for managements complications like resp. depression, severe pruritus,
Dose- 1 to 5μg/kg or 0.1 to 0.4 mg given slowly IV continuous infusion 5μg/kg/hr. duration 30-45 min. Intramuscular twice dose, longer effect.
Guidelines for use of narcotic analgesics
- Start specific drug for specific type and severity.
- Know the pharmacology well
- Adjust the dose and route as per patient’s need and comfort.
- Use drug combination for additive effects and reduce side effects
- Anticipate and treatment side effects
- Watch for development of tolerance and addiction etc.
- Prevent acute withdrawal by slow tapering.
- Anticipate and manage complications like overdose etc.
C] Adjuvants analgesics
Adjuvant analgesics are defined as drugs with a primary indication other than pain that have analgesic properties in some painful conditions. They are useful as coanalgesics, Counter acts side effects like nausea, vomiting, constipation etc. Take care of associated symptons like depression, insomnia, loss of appetite.
Classification of adjuvants analgesics :Based on the etiopathology of pain they are
- Drugs potentially useful for any type of pain-multipurpose coanalgesics.
- Drugs used for treatment of neuropathic pain.
- Drugs used for bone pain.
- Drugs used for pain and other symptoms in the setting of bowel
obstruction. - Drugs used for musculoskeletal pain.
| I. Multipurpose Analgesics | ||
| a) | Antidepressants | |
| Tricyclic Antidepressants | Tertiary amines – clomipramine, imipramine, amitryptiline,doxepin | |
| Secondary amines – Nortryptyline, desipramine | ||
| Selective Serotonin reuptake inhibitors(SSRI) | Paroxetine , Citalopram | |
| Noradrenaline / Serotonin reuptake inhibitors. (SNRI) | Venlataxin, Duloxetine, Minalcipran | |
| Others | Bupropion | |
| b) | Corticosteroids | Dexamethasone, Prednisolone, Predinisone, Betamethasone |
| c) | ά 2 adrenergic agonists | Clonidine, Tizanidine |
| d) | Neuroleptics | Olanzipine |
| II. For Neuropathic Pain | ||
| b) | Anti convulsants | Gabapentin, Pregabalin, Carbamazepine, topiram, lamotrigine,levetiracetam,oxcarbazepine,tiagabine,Zonisamide, Phenytoin Sodium, Valproid acid |
| C) | Local Anesthetics | Lignocaine ,Mexiletine |
| d) | N- Methyl-D-Aspartate receptor antagonists | Ketamine, Dectrome- thorphan, memantine, amantidine,Newer-Flupiritine |
| e) | Other | Baclofen,Cannabinoids, PsychostimulantDrugs methylphenidate, metadata, modatinil |
| f) | Topical Drugs | Lignocaine,Prilocaine ,Capsaicin etc |
| III. For bone pain | |||
| a) | Corticosteroids | Dexamethasone, Predisone | |
| b) | Calcitonin | ||
| c) | Bisphosphonate | Pamidronate,Zoledronic acid,clodronate etcStrontium, Samarium | |
| d) | Radiopharmaceuticals | Strontium,Samarium | |
| IV. For Musculoskeletal Pain | |||
| a) | Muscle relaxants | Baclofen,Tizanidine,Cyclobenzapine, Orphenadrine,Carisoprodol, Metaxalone Methocarbol, | |
| b) | Benzodiazepines | Diazepam, Lorazepam Clonazepam | |
| V. Adjuvants for pain from bowel obstruction | |||
| Octreotide | |||
| Anticholinergics | Scopolamine,glycopyrolate | ||
INTERVENTIONAL PAIN MANAGEMENT
Definition: Interrupting the transmission of pain signals to decrease the level of discomfort experienced without the need for invasive surgery or the total reliance on potent prescription medications.
It is one of the multimodal approaches and is mainstay in the management of moderate to severe chronic cancer pain for adequate & long term pain relief.
Indications
- Immediate relief of uncontrolled pain (meanwhile opioids started)
- Transient blockade for positional pain & planned for procedure.
- Longer duration blockade when no relief with routinenon invasive
procedures
Two Main Types interventional pain management techniques :-
- Augmentative :- Infusional techniques, Electrical stimulation techniques
- Ablative :- Blocking nociceptive(pain) transmission by, Neurolytic
procedures, Radiofrequency denervation , Cryoanalgesia etc
A] Augmentative Methods
IV infusion – Gives immediate relief in acute pain. used as Continuous infusions with PCA pumps, Infusion pumps, Mechanoelastic pumps etc e.g. Fentanyl 0.5-1 mgm/kg/hr, Tramadol 50-100 mg/24 hrs.
Limitations:- CNS effects – sedation, myoclonus, confusion respiratory,circulatory depression etc.
Subcutaneous Infusions:- It is a Safe, simple , cost effective alternative to i.v. infusions. Drugs uesd are morphine , hydromorphone , methadone, fentanyl , sufentanyl.
Morphine – 5mg per ml , hrly rate not more than 2ml per hr.
Weekly site change required
Sites – chestwall or truck ide
Intracerebroventricular Infusion:- Given through intracerebroventicular cathetors tunneled & connected to reservoir or port.
Indications – Severe refractory head and neck cancer pain with 1-3 months survival time.
Morphine-Increased potency through this route.
Dose – Initial 0.25mg to 2mg, Onset – 2 to 30 min. , Duration – 12 to 48 hrs.
Side effects – Risk of respi. depression, first 3 days,Infections,CNS effects Ref. :Obbens , E.A.M.T. et al , PAIN 28:61,1
Intraspinal Analgesia:- It is To be included in comprehensive treatment plan of cancer pain managements. Is used After adequate trial of systemic opioid & adjuvs
Indications –
- Moderate-severe degree pain during primary antineoplastic treatment.
- Patients with severe movement related pain
- Pain emergencies
- Chronic survivors, Short life expectancy(DDS)
- With more wide spread area of Pain
Different Agents Used:- Opoids- Morphine, fentanyl, hydromorphine, sufentanyl.
Local anaesthetics- Bupivacaine, Lignocaine, Tetracaine Clonidine ( Alpha 2 receptor agonist) Ketamine ( NMDA antagonist) Tramadol Ketorolac (Cox-1,2 inhibitor) Baclofen (Gaba agonist for spasticity), Ziconotide ( Ca+ channel inhibitor).
Mechanism Of Action of intraspinal analgesics :
- Opioids Analgesia primarily due uptake of opioids into spinal cord and
CSF. Effects both pre and post synaptically by reducing neurotransmitter
release and hyperpolarising the membranes and inhibiting pain. - Local anesthetics act by inhibiting the sodium channel (Epidural use)
- Clonidine is an alpha-2 agonist that depresses release of C fiber
neurotransmitters, Substance P and Calcitonin Gene Related Peptide (CGRP).
Approved for epidural use. - Ziconotide is a calcium channel inhibitor specific to the dorsal horn of
the spinal cord - Baclofen a GABA agonist, used in spasticity to restore balance between
active and passive muscles
Spinal Drug Delivery Systems:- These are the systems used to deliver different drugs into the epidural or intrathercal space. The systems comprises:- Spinal cathetors, Subcutaneous reservoirs for intermittents injections, Implanted infusions pumps with constant rate or programmeable rate.
Nerve Blocks :
To determine source of pain pathways (Somatic or sympathetic) e.g. intercostal/epidural, Prognostic to predict outcome of permanent interventions like numbness, motor block & other side effects of neurolysis or rhizotomy ,Pre-emptive to prevent painful sequelae e.g Phantom limb or causalgia. Therapeutic to treat painful conditions that respond to nerve block (e.g. celiac block for pancreatic pain).
Imaging or nerve locator guidance is used for better accuracy in various nerve block procedures, with the help of advances in technology in last two decades.Better precision achieved with Fluoroscopy guidance , Nerve locator guidance ,Simulator fluro guidance, CT guidance ,CT – Robotic intervention,Ultrasonography guidance etc.
Different nerve blocks used in cancer pain management
- Head and Neck region -Gasserian ganglion block, Mandibular & , Stellate
g.-repeated/ continuous, Cervical epi./paraverte-Neurolytic
Glossopharyngeal,Sphlenopalatine etc. - Thoracic pain – Intercostal nerve block-3-6% phenol or25-50%
alco./pulsed RF, Thoracic epidural/subarachinoid block, Interpleural block
T2-T3 Neurolytic,pulsed RF, Thoracic paravertebral etc. - Upper abdominal pain – Thoracolumbar region- Epidural, Subarachnoid,
Paravertebral ,for Visceral pain- Lower intercostal nerve block ,CELIAC
PLEXUS BLOCK , Splanchnic etc. - Abdominopelvic pain –Lumbar region Epidural ,Subarachnoid ,Lumbar
sympathetic, superior hypogastric ,Sacral Nerve block,Caudal block,Ganglion
Impar etc. - Upper extremities- Stellate,T2-T3 ganglion block,Brachial plexus block
,Peripheral nerve blocks etc. - Lower extremities-Lumbosacral- Epidural,Subarachnoid,Lumbar sympathetic
,Peripheral nerve blocks
Neurolytic(chemical) Blocks
Indications
- Indicated in severe persistent pain.
- Indicated for relatively localised pain.
- In patients with short life expectancy.
Prerequisites
- Inform and discuss the risk benefit ratio with family members.
- Prior 1/2 diagnostic blocks with local anesthetics recommended.
- Assess the results of L.A. block and then proceed.
Commonly used neurolytic Blocks
- Spinal Neurolysis-Subarach./epidural
- Paravertebral block
- Sympathetic Blocks- Stellate ganglion,T2-T3,Splanchnic plexus,Celiac
plexus ,Sup. Hypogastric plexus,Ganglion of impar ,Lumbar sympathetic etc. - Diff.ganglion & Nerves- Trigeminal ganglion, & Mandibular, Maxillary
nerve , Glossopharyngeal, Intercostal etc.
Spinal Chemical Neurolysis:- It is an Effective method of pain control In cancer Patients with limited life expectancy.
Used for Pain over 2-3 layers of dermatomes (esp. Sacral,perineal & thoracic region)
Advantages of the techniques
- High proportion of good results in properly selected patients.
- Ease of performance with minimal equipment.
- Minimal or no requirement of hospitalisation.
- Duration of relief adequate for preterminal.
- Ease of repetition.
- Suitable for aged and debilitated.
- Low complication rate with proper techniques
Subarachnoid Neurolysis
Subarachnoid neurolysis -Ethyl alcohol conc.97%,approxi.0.2 to 2 ml in 0 .1ml aliquote used.
Indications- Intractable pain below head / Pain relief better & longer lasting
Complications- Minimal with Proper selection, Preparation, Positioning for post rootlets & Precision of technique. Majority of complications subside within few weeks.
Epidural Phenolisation- 6 % – 8% aqueous phenol , Approx. 1.5ml/dermatome bilateral
Advantages over subarachnoid :
- Less risk of meningeal irritation
- Less spread of solution to cranial nerves
- Less risk of bladder, bowel involvement
- More applicability for widespread bilateral pain
- Less chances of spread to anterior roots
- Less chances of postdural puncture headache
References for neurolysis :
- For Neck Pain Cathetor inserted at C7-T1 level & advanced 4-5 cms.
Cathetor placement Checked with epidurogram (Contrast Spread) or Checked
with 1% Xylocaine 2ml -> Neurolytic 2 hrs. after total dose of L. A. - RACZ -5.5% Phenol in Saline
(Racz repeated epidural phenol injection in chr. Pain & spasticity.
In Persistent pain: Morden methods of treatment, Vol 5 edited by S. Lipton,
New York, Grune & Stratton. 1985 PP 157 – 180)
Recent techniques of pain management
- Radiofrequency ablation (RF):- Neurolysis by
thermocoagulation /RF Lesion with high frequency current passed down a
thermocouple probe, passed through insulated canula.
Two types of RF are Conventional RF and Pulsed RF
Fluoro/CT Guidance used for better accuracy
Indications:- for Radiotherapy(RF) Lesioning in cancer pain
Peripheral nerve RF- Gasserian gangllion ,trigeminal branches Maxillary,
Mandibular, Supraorbital, Infraorbital etc., Suprascapular, Intercostal,
LCNT,stellate gangllion,splanchnic,Lumber symphatetic etc.
Advantages of Rf Lesioning-Long lastin effect- Minimaly Invasive percutaneous procedure.
- Lesion size can be accurately controlled without damage to adjacent
strs - Accurate placement of with sensory ,motor stimulation, impedance
measurement
- Vertebroplasty:- Percutaneous augmentation of vertebral
body using polymethyl methacrylate.
Indications:– Compression fractures caused by osteolytic Vertebral mets,
osteoporosis, vertebral angiomas,
Severe back pain due to vertebral collapse
In Metastases and myeloma radiotherapy follows.
Interventional Pain Procedures : Year 2010-2011
RST Regional Cancer Hospital, Nagpur ,(Total procedures n=138)
| Sr. No. | Name of Nerve Block | No. of Patients | % of procedure (Total procedures , n=138) |
|---|---|---|---|
| 1 | Mandibular/ Maxillary | 54 | 39.13 |
| 2 | Stellate (repeated) | 32 | 23.19 |
| 3 | Coeliac plexus block (CT/fluro) | 14 | 10.14 |
| 4 | Lumbar sympathetic | 9 | 6.52 |
| 5 | Subarachnoid alcohol | 5 | 3.62 |
| 6 | Superior hypogastric | 5 | 3.62 |
| 7 | Epidural phenolisation | 4 | 2.9 |
| 8 | Trigeminal (steroid) | 4 | 2.9 |
| 9 | Epidural DDS | 4 | 2.9 |
| 10 | Paravertebral | 4 | 2.9 |
| 11 | Glossopharygeal | 3 | 2.17 |
| 12 | Total | 138 | 100 |
Interventional Pain Procedures : Year 2013-2014 RST Regional Cancer Hospital, Nagpur (Total new patients seen n=724.Total procedures n=235)
| Sr. No. | Name of Nerve Block | No. of Patients | % of procedure (Total procedures , n=235) | % of procedure (Total no. of OPD patients ,n=724 ) |
|---|---|---|---|---|
| 1 | Mandibular Neurolytic | 65 | 27.66 | 8.98 |
| 2 | Thoraco Lumbar Phenolisation | 44 | 18.73 | 6.08 |
| 3 | Stellate Ganglion | 38 | 16.17 | 5.25 |
| 4 | Trigeminal Ganglion | 19 | 8.09 | 2.62 |
| 5 | Coeliac Plexus | 14 | 5.96 | 1.93 |
| 6 | Lumbar Paravertebral | 11 | 4.68 | 1.52 |
| 7 | Cervical Epidural Phenolisation | 7 | 2.98 | 0.97 |
| 8 | Lumbar Sympathetic Neurolysis | 7 | 2.98 | 0.97 |
| 9 | Superior Hypogastric plexus | 7 | 2.98 | 0.97 |
| 10 | Subarachnoid neurolysis | 6 | 2.55 | 0.83 |
| 11 | Glossopharyngeal N.block | 5 | 2.13 | 0.69 |
| 12 | Cervical Paravertebral | 4 | 1.7 | 0.55 |
| 13 | Maxillary N.block | 4 | 1.7 | 0.55 |
| 14 | Epidural Drug Delivery System | 4 | 1.7 | 0.55 |
| 15 | Total | 235 | 100 | 32.46 |

