
Managing Chronic Pain

– Dr. Chandrashekharan Cham
MBBS DA FIPM
Consultant Anaesthesiologist and Pain Physician
MBBS DA FIPM
Consultant Anaesthesiologist and Pain Physician
MANAGING CHRONIC PAIN
Introduction:
“PAIN is a more terrible lord of Mankind than even death itself” is written in the front page of the book by Nobel Laureate Albert Schweizer in 1931. (“Bonica’s management of pain” published in 1953).
Pain is a latin word Pheona means punishment. According to Christianity pain is a curse given by god to human beings and need no attention. That is why, even though pain is as old as mankind, treatment of pain got its importance probably only after 1930.
Evolution:
John Bonica, the founding father of interdisciplinary pain care, was the key person in initiating pain management and also instrumental in formation of the International Association for the Study of Pain (IASP) in 1984.
IASP Definition of Pain (1984)
“An unpleasant sensory and emotional experience associated with actual or
potential tissue damage, or described in terms of such a damage”
The American Board for Hospital Accreditation defines pain as 5th vital
sign along with the other vitals like pulse, blood pressure, respiration, temperature
and incorporated pain monitoring in each hospital vital monitor chart.
Why should pain be treated?
While acute pain is a protective physiological condition, chronic pain is a pathological condition, disease state. It should be treated as early as possible because it causes sleep disturbance, depression, anxiety, decreased quality of life leading to disruption of daily routine, reduced social activity, disability, work related problems and not least of all the health care costs.
Various types of chronic pain are treated in pain centers like –
- Low back pain
- Complex regional pain syndrome
- Trigeminal neuralgia
- Fibromyalgia
- Painful Diabetic Polyneuropathy
- Refractory cardiac angina
Management of chronic pain: Multidimensional approach
Chronic pain is multidimensional in nature, thus its management should be multimodal and interdisciplinary. Current approaches recognize the value of a multidisciplinary treatment framework that targets not only nociceptive aspects of pain but also cognitive-evaluative and motivational affective aspects and intend to reduce sequels of pain. The interdisciplinary management of chronic pain typically includes multimodal treatments such as: non-pharmacological modalities like psychological therapy, physical therapy, behavioral therapy; pharmacological modalities like combinations of analgesics and co-analgesics; interventional pain management and also the surgical options.
The multimodal approach more adequately and comprehensively addresses pain management at the molecular, behavioural, cognitive-affective and functional levels.
Pharmacological approaches
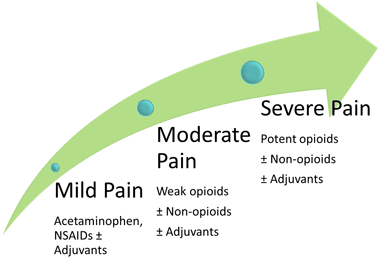
WHO Ladder of analgesic therapy:
The WHO 3-Step Ladder for Pain Management is an important guideline of analgesic therapy in both cancer and non-cancer pain. It is not a rigid and compulsory instrument but still in use since 1996. When initiating analgesia, classically – for mild pain start at step one, for moderate pain step two, for severe pain step three. If there is not pain relief, maximize the dosing at the current step and then, if this is insufficient, move up the ladder.
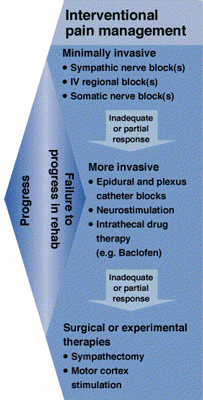
Interventional pain management
-
 Diagnostic medical branch blocks or facet injections may be considered for patients with suspected facet mediated pain to screen for subsequent therapeutic procedures.
Diagnostic medical branch blocks or facet injections may be considered for patients with suspected facet mediated pain to screen for subsequent therapeutic procedures. - Diagnostic sacroiliac joint injections or lateral branch blocks maybe considered for the evaluation of patients with suspected sacroiliac joint pain.
- Diagnostic selective nerve root block maybe considered to further evaluate anatomic level of radicular pain.
- The use of sympathetic block maybe considered to support the diagnosis of sympathetically maintained pain.
- Peripheral block maybe considered to assist the diagnosis of pain in a specific nerve distribution, e.g. Trigeminal neuralgia, glossopharyngial neuralgia, brachial plexus injury.
- Provocative discography maybe considered for the evaluation of selected patient with suspected discogenic pain.
- Radiofrequency ablation of the medial branch nerves to the facet joint, trigeminal ganglion for neuralgia, stellate ganglion for CRPS of upper limb, sphenopalatine ganglion for headache, splanchnic plexus for abdominal pain can be performed.
- Celiac plexus blocks using local anesthetics with or without steroids maybe used for the treatment of pain secondary to chronic pancreatitis.
- Lumbar sympathetic blocks or stellate ganglion blocks may be used as components of the multimodal treatment of CRPS if used in the presence of consistent improvement and increasing duration of pain relief.
- Botulinum toxin maybe used as an adjunct for the treatment of piriformis syndrome.
- Spinal cord stimulation: This may be used in the multimodal treatment of persistent radicular pain in patients who have not responded to other therapies. Spinal cord stimulation may also be considered for other selected patients (e.g. CRPS, peripheral neuropathic pain, peripheral vascular disease, and postherpetic neuralgia).
- Epidural steroids with or without local anesthetics: Epidural steroid injections with or without local anesthetics may be used as part of a multimodal treatment regimen to provide pain relief in selected patients with radicular pain or radiculopathy.
- Intrathecal non-opioid injections: Ziconotide infusion may be used in the treatment of a select subset of patients with refractory chronic pain.
- Intrathecal opioid injections: Intrathecal opioid injection or infusion may be used for neuropathic pain patients. Neuraxial opioid trials should be performed before considering permanent implantation of intrathecal drug delivery systems.
- Minimally invasive spinal procedures (e.g.vertebroplasty) may be used for the treatment of pain related to vertebral compression fractures.
Choosing an option
Choosing an option should be individually tailored, according to patient indications and expectations having in to account the cost and benefit of treatment. All patients with chronic pain should have a documented history and physical examination and an assessment that ultimately supports a chosen treatment strategy.
Summary
- Pain is a serious health problem, and imposes a great burden on the lives of patients and their families.
- A step ladder approach or following a Pain continuum is the ideal approach.
- Advanced Interventions are mandatory when all conventional modalities fail.
- Emphasis is on the Quality of Life than just pain relief.

