
A Case Report of 11yr Old Child

– Dr. Sheetal Dalal
Associate Professor, Dept of Anesthesia, IGGMC, Nagpur
Associate Professor, Dept of Anesthesia, IGGMC, Nagpur
Persistent Ventricular Bigeminy during Anaesthesia in Paediatric Patient – A Case Report of 11yr Old Child
Dr. Sheetal Dalal (Associate Professor),
Dr. Vikas Chaudhari (Assistant Professor)
Department of Anaesthesiology IGGMC, Nagpur

Abstract
11year old male child with fracture of both bone forearm left side posted for open reduction and internal fixation. Pre-anaesthetic check-up and investigations did not revealed any pre-existing underlying cardiorespiratory disease. Patient had uneventful perioperative period one day prior in emergency hours during closed reduction. Patient was comfortable without any anxiety or restlessness. After uneventful induction and intubation as per routine protocol , patient received Injection (Amoxicillin plus clavunate) 600mg Intravenously as an antibiotic and after 3min patient developed Persistent ventricular Bigeminy with intermittent sinus rhythm, regained to normal after 20mins.Open reduction and internal fixation of fracture both bones was done. Extubation and postop course was uneventful. To rule out cause of arrhythmia, ECG, 2D-ECHO & serum electrolyte were done but it was normal.
Patient again had fall on same hand and revisited ortho OT for revision surgery. As child was very co-operative and calm, patient was given supraclavicular block after proper counselling. After 30 mins before tourniquet inflation as a routine method, Inj. (Amoxicillin plus clavunate) 600mg was given. After 5mins patient developed Persistent ventricular Bigeminy. After 1hour child complained of chest pain and had redness of eyes and restlessness. It was managed with 100% oxygen and Injection Amiodarone 150mg intravenously and surgery was postponed for further stabilization and optimization. Serum Electrolytes were normal. Child was observed in Surgical Intensive Care Unit with continuous ECG monitoring. Ventricular Bigeminy with intermittent sinus rhythm persisted for 3 days. It was managed with Tab. Metaprolol 12.5mg BD and Tab. Amiodarone 100mg OD. Paediatric cardiologist opinion was taken & repeat 2D-ECHO revealed no abnormality. After 5 days, patient was discharged and surgery rescheduled after 2 weeks with continuation of Tab. Metaprolol and Tab. Amiodarone. During fourth time we avoided Injection (Amoxicillin plus clavunate) and all anaesthetic drugs which might have contribute to cardiac arrhythmias. The perioperative period was uneventful. An in depth discussion of the case and ventricular dysrhythmias in paediatric population is emphasized in this case report.
Keywords- Paediatric Cardiac Arrhythmias, Ventricular Bigeminy, Management of Paediatric Arrhythmias
Introduction
The overall incidence of arrhythmias is 13.9% among 100,000 emergency room visits and 55.1% 100,000 paediatric emergency room visits (children under 18 years of age).1
The present case report will focus on ventricular dysrhythmias specially Premature Ventricular Complexes (PVC’s) in paediatric population. PVCs are premature depolarisation of ventricle leading to early, less co-ordinated, systolic contraction of ventricles and routinely have compensatory pause that follows them. PVCs commonly occur in infancy, decline in incidence in early childhood and become increasingly common again in adolescence and adulthood.2, 3
The most common cause of ventricular dysrhythmias during general anaesthesia is light plain of anaesthesia, hypotension, hypoxia, hypercarbia, electrolyte disturbances, apprehension & anxiety in paediatric population. But many patients are symptomless and comfortable with stable vitals with underlying ventricular bigeminy with intermittent sinus rhythm.2, 3 Injection (Amoxicillin plus clavunate) is routine antibiotic of choice for surgical procedures and incidence of ectopics is reported in age of 10-19yrs is 1.67% 4, 5, 6 The main aim to present this case report is how to approach such patient systematically and precaution to be taken for successful management. This case report also emphasizes on documentation and counselling of patients required to avoid future sequel.
Case presentation
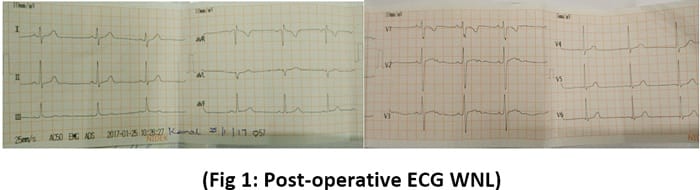
An 11 year old child weighing 35kg was posted for fracture of both bones left forearm for open reduction and internal fixation. Pre-anaesthetic check-up was done. He had history of fall while playing for which he underwent closed reduction under general anaesthesia two days back during emergency hours. Perioperative period was uneventful and there was no history pertaining to any underlying major disease. His routine investigations were under normal limits.( Hb- 12.3gm%, TLC/DLC-WNL, Blood Sugar- 95mg%, Serum Creatinine- 0.6mg%,Urea-18mg%, Na+-139mEq/lit, K+-4.5mEq/lit Liver Function Test-WNL, chest X-ray-WNL) Blood group was B negative. On table, his Pulse rate -80/min, regular, Blood pressure – 110/70mmHg, ECG showed normal sinus rhythm and Oxygen saturation – 98%.Intravenous line was established and child premedicated with 0.75mg of midazolam, 50µgm of fentanyl, 20µgm of glycopyrolate. After pre-oxygenation for 3mins, induction done with intravenous Propofol 70mg and suxamethonium 70mg. Patient was intubated with cuffed ET tube no. 6.0 and anaesthesia was maintained on oxygen plus nitrous oxide plus sevoflurane, and atracurium was used as muscle relaxant. Injection (Amoxicillin plus clavunate) 600mg was used as antibiotic prophylaxis and after 3mins, monitor showing persistent ventricular bigeminy with intermittent normal sinus rhythm but rest of parameters were normal. Depth of anaesthesia increased and sample was sent for serum electrolytes and it was within normal limits. Ventricular bigeminy continued for 30 mins. and regained normal sinus rhythm. Internal fixation of both fractures was done. Child was extubated and kept under observation for ECG monitoring for 24 hours but uneventful and discharged. For total evaluation of cardiovascular system, Post op ECG (fig 1) and 2 D- ECHO were done but it did not reveal any significant changes.
After 1month child again had a fall on same side and had same fracture and patient was posted for revision surgery. Pre-anaesthetic check-up and investigation were within acceptable limits. The child was very comfortable, he had no anxiety or restlessness. Anaesthesia plan was to do surgery under brachial plexus block using supraclavicular approach and procedure was explained to patient and mother. After establishing intravenous line monitors were attached. ECG and all vital parameters were within normal limit. Under all aseptic precautions supraclavicular block was given with Peripheral Nerve Stimulator with 35mm stimulating needle by injecting 10cc 0.375% of bupivacaine and 10cc of 1.5% lignocaine with adrenaline. After achieving anaesthesia within 20mins tourniquet was applied. Inj. (Amoxicillin plus clavunate) 600mg was used as antibiotic prophylaxis. Within 3min after antibiotic injection child again developed persistent ventricular bigeminy with intermittent sinus rhythm. (Fig 2).
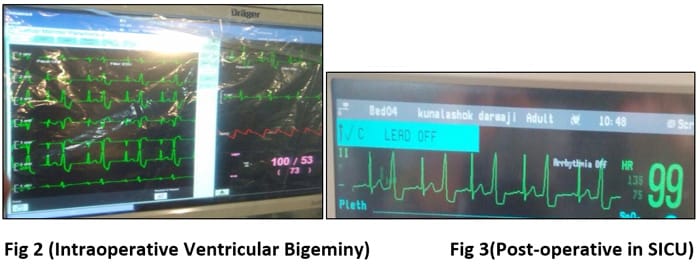
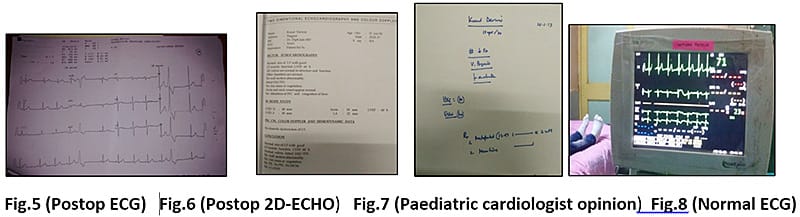
Surgical procedure was abandoned. It was managed by Inj. Hydrocortisone 60mg and Inj. Avil and Inj. Xylocard 60mg intravenously. Oxygen supplemented on ventimask. Other vitals were normal. But ventricular bigeminy persisted. After 1hour child complaint of chest pain and he had redness both eyes and became restless. 100% O2 was supplemented on mask and Inj. Amiodarone 150mg slowly over 10mins. Continuous bigeminy converted to normal sinus rhythm with intermittent ventricular ectopics. Serum electrolyte were within normal limit. Child was comfortable and shifted to surgical intensive care unit for continuous ECG monitoring. Tab. Metaprolol 12.5mg started twice a day. The child had frequent changing patterns of ectopics and bigeminy for 2 days. (Fig 4 & 5) Again Tab. Amiodarone 100mg once a day was added.
Bigeminy pattern persisted for 5 days with stable hemodynamics. The child was comfortable all the time. Child was referred to paediatric cardiologist for complete cardiac evaluation. Repeat 2D- ECHO was done and report was normal (FIG 6 & 7) and cardiologists continued Tab. Metoprolol and tab. Amiodarone for 2weeks. ECG showed normal sinus rhythm. (Fig 8)Electrophysiological study was advised but could not possible due institutional & financial limitation. After optimization patient was taken for revision surgery. As patient was not ready for regional anaesthesia general anaesthesia was planned. At that time we deliberately avoided Inj. (Amoxicillin plus clavunate) and Inj. Cefotaxim was used as antibiotic in view of (Amoxicillin plus clavunate anaphylaxis) i.e. (Amoxicillin induced Ventricular Bigeminy). The child was premedicated with Inj. Glycopyrrolate 0.1mg plus Inj. Midazolam 0.75mg and Inj. Fentanyl 50µgm intravenously. Induction done with Intravenous Propofol 70mg and Rocuronium 30mg and intubated and anaesthesia was maintained on oxygen and Isoflurane and Inj. Vecuronium with intermittent Fentanyl. Intraoperative vitals were absolutely normal with normal ECG sinus rhythm. Internal fixation of both fractures was done.Extubation and postoperative period was uneventful. Patient was discharged after 2 days with instructions to mother not to give (Amoxicillin plus clavunate) in any form in future. He was advised to undergo electrophysiological study to avoid future sequel.
Discussion
PVC’s are not uncommon finding in healthy paediatric population. PVC’s are more common in arena of anaesthesiology because of multiple agents used in anaesthesia practice which have a direct effect (sympathomimetic, volatile anaesthetics) or an indirect effect (light plain of anaesthesia, pain, ketamine) on hearts conduction system. It is imperative that anaesthesiologists understand the context of when PVC’s during anaesthesia can become life threatening and require further investigation and referral. Although most children who have PVCs or can be associated with underlying heart disease, MVP, prolonged QT syndrome, cardiomyopathies (dilated and hypertrophic ), electrolyte imbalance, drug toxicities, hypoxia.1
History is crucial factor in ascertaining which cardiac arrhythmias are significant or benign. Important elements include history of palpitation, syncope and chest pain and family history. Referral to paediatric cardiologist is essential where patient is asymptomatic, the diagnosis is new or ECG demonstrates a significant abnormality.2,3,4
Holter monitor provides continuous rhythm recording from adhesive electrode for a minimum of 24-48 hours. This monitor provides information regarding minimum/average/maximum heart rate, longest pause, the number of pre-atrial contractions and PVCs and the number of SVT and ventricular tachycardia. This is useful monitor for children who are symptomatic with irregular heart rate or symptomatic child to isolate arrhythmias during onset of symptoms.2,4
Exercise testing is a noninvasive way to observe the effect of enhanced sympathetic drive in children with an ECG or Holter monitor abnormality.2
ECG is mandatory and 2D-ECHO should be done where there is suspicious of cardiac structural disease. Electrophysiological study may be required to provide a more definitive etiology and diagnosis if previous study failed to diagnose Furthermore some arrhythmias (certain SVTs and VTs) can be mapped and ablated during this invasive study.
PVCs can also appear regularly as a part of organised rhythm called “ventricular parasystole”. If not treated timely chances of developing sustained dangerous (VT with pulse) or deadly (VT or ventricular fibrillation without pulse) is higher.5
Anaesthesia on its own contributes to PVC’s due to hypoxia, tachycardia, hypertension, hypercarbia leading to imbalance between myocardial O2 supply and demand leading to ectopic ventricular rhythm in paediatric population. Anaesthesia management of PVC’s are noted above to establish causes and treat the most likely diagnosis once life threatening presentation addressed. Β blockers are the most successful drug for suppressing intermittent ventricular ectopic especially with tachycardia and should be first line of treatment while lidocaine and amiodarone should be reserved for cases where PVCs progress to run VT or Persistent ventricular tachycardia. Early defibrillation or cardioversion indicated depending on pulse.3
Whenever Persistent ventricular ectopic rhythm is observed intra-operatively, the anaesthesiologists should monitor the patient during recovery phase and consider urgent or early evaluation if dysrhythmias persist once anaesthesia medication has been eliminated to reasonable degree. Surgery should be cancelled and cardiac consultation and cardiac stabilization done before rescheduling of patient for surgical procedure.
A survey by FDA reported several articles about antibiotic induced arrhythmias. These antibiotics cause changes in electrical activity of heart & also can lead to electrolyte disturbances leading to arrhythmias which may be fatal if not treated. Increase incidence were reported with underlying cardiac abnormalities. In Jan 2004 to Oct 2012, a survey was carried out about Amoxicillin induced other side effects and arrhythmias. They concluded that there were 0.8722% incidence of arrhythmias due to Amoxicillin.6,7,8 .In the study carried out by Criticare med in 2010 on (Amoxicillin plus clavunate) induced heart palpitation,the incidence palpitation and irregular cardiac rhythm in the age 10-19 yrs was 4.35%. though it is popular antibiotic.
Treato Update & ehealth me stated in update March 2017, that Amoxicillin causes irregular heartbeat.
Recently FDA has carried out large study, out of 32879 people have side effects, and 480 people (1.46%) have irregular heartbeat. Incidence of arrhythmias <1mth is 98.33%, 1 to 9yr of age is 0.26% &10-19yrs is 2.04%.9, 10, 11
In our case patient did not receive any antibiotic during first exposure to anaesthesia for closed reduction and perioperative period was uneventful. During second exposure to general anaesthesia developed Persistent ventricular Bigeminy after Inj. (Amoxicillin+ clavunate) but regained sinus rhythm within 2 hours. So we thought it might be due to anaesthetic drug or light plain of anaesthesia or underlying silent cardiac abnormality which we might have missed during preanaesthetic check-up. So to rule out underlying cause ECHO and 24hr ECG monitoring done but did not reveal any abnormality. During the third exposure child was very co-operative and comfortable and was given supraclavicular block and he again developed ventricular bigeminy, chest pain and redness of eyes after Inj. (Amoxicillin+ clavunate) but severity was more and treated with β blocker and amiodarone. It took 6-7 days to regain normal sinus rhythm.
Patient was referred to paediatric cardiologist and 2D-ECHO was done which were normal. We advised electrophysiological study but not possible due to Institutional & financial limitation. We optimized the patient for 2 weeks and rescheduled the surgery. During fourth exposure to anaesthesia, we avoided Inj. (Amoxicillin+ clavunate) all anaesthetic drugs which may contribute to cardiac arrhythmia. The perioperative period was uneventful. So we stated that the ventricular ectopics may be due to (Amoxicillin+ clavunate) induced but confirmatory diagnosis yet to be established as electrophysiological study could not be performed.
Patients parents were instructed about sensitivity to (Amoxicillin+ clavunate) and documentation was done on discharge card. He was advisedto undergo electrophysiological study to avoid any future sequel.
Conclusion
Anaesthesiologists are likely to encounter cardiac rhythm abnormalities during anaesthesia. There are no clear guidelines or algorithm or protocol for detection of cardiac arrhythmias in paediatric population. The most common recommendation is determination of underlying cause to avoid life threatening event. Primary care physician, detailed history, 12 lead ECG mandatory, referral to paediatric cardiologist is necessary, Holter monitoring ,exercise testing, ECHO and electrophysiological intervention are all available aids.
References-
- Doniger S.J.,Paediatric dysarrythmias:Pediatr clin N.Am.2006 ;53:85-105
- Blaufox AD:Irregular hrt rate (arrhythmias) in children. In: Triedman JK, Armby C, eds uptodate : Waltham ,Mass,Accessed September 4, 2012
- Walson KT,Abnornmalities of cardiac conduction and cardiac rhythm In: Hines RL, Marshal KE eds Stolteing’s Anaesthesia & Co Existing Disesase : 5th edition Philadelphia: Pa: Churchill livingstone 2008:61-86
- Bryan Neil at all; 13 yr old girl in trigeminy during anaesthesia for outpatient dental anaesthesia: A case report Anaesth prog 62; 110-113 2015
- Dubin D Rapid Interpretation of EKG’S.6th ed Tampa.Fla:Cover publishing 2000
- Drug induced arrhythmias Criticare med 2010
- Abo-salem E,Flower JC et al :Antibiotic Induced cardiac arrythmias ,Cardiovasc Ther 2014 Feb 32(1):19-25
- Katie Glenn American college of cardiology,common antibiotics increase risk of cardiac arrythmias, cardiac death, Nov o9,2015
- Amoxicillin & Heart Palpitation –From FDA Report: ehealth me Feb 26, 2017 & March 2017
- FDA:Popular antibiotic can cause fatal heart rhythums : CNN Staff updated, March 2013
- Treato:Does Amoxicillin cause palpitation?Last update March 11,2017
