
‘ORGAN’ized Life Saving

Dr. Neeta Deshpande
Consultant Anesthesiologist
and Incharge Emergency Medicine
Orange City Hospital and Research Institute
Nagpur
Human to human transplantation of organs has been accepted by healthcare professionals as the best and often the only cure for a wide range of fatal diseases.
Cadaver donors are the sole source of organs for extra-renal transplantation & remains an important source of kidneys for renal transplantation. Although donation after circulatory death (DCD) is also very important, particularly for kidney transplantation, currently most transplants follow multiple organ retrieval from heart beating donors after brain death (DBD).
Experts say that the organs from one donor can save as many as 8 (eight) lives.
However, organ donation is yet to make a significant dent in India…. Be it ignorance, lack of knowledge, myths about organ donation, traditional beliefs particular to Indian society or failure to record one’s wish for organ donation, there is a vast gap between the number of organs donated and the people waiting for organ donation is getting larger. Some disturbing statistics around the same are as follows:
- Almost 1.75 lakh people in India need a kidney; but less than 5000 receive one.
- 90% of people in the waiting list die without getting an organ.
- India’s annual liver transplant requirements is over 100000, but we manage only about 1000.
- 70% liver transplants are taken care of by a live donor, and only 30% are dependent on cadaver donors.
- Annually around 50000 hearts and 20000 lungs are required.
DATA OF DOD FROM ZTCC NAGPUR
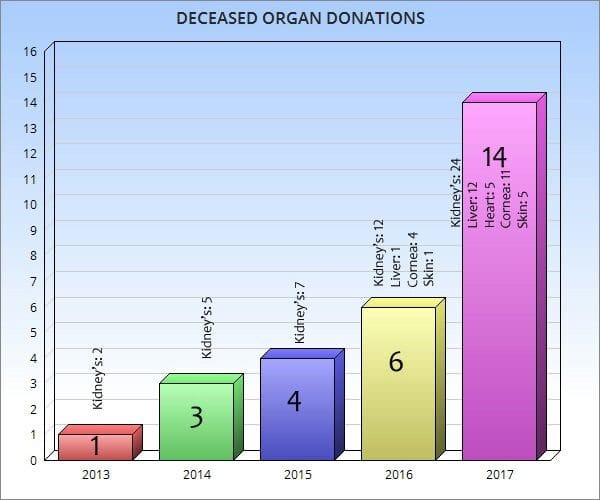
Statistics from Orange city Hospital:
Since 2015, we have retrieved organs from6 cadavers – in 2015, 2 patients were taken for kidney retrieval and one kidney transplant from each cadaver took place in OCHRI itself.
In 2016, one cadaver was taken in OT and both the kidneys were sent outside, as our own KT, team was not available.
In 2017, 3 cadavers underwent organ donation and we could retrieve 3 livers, 1 heart, 6 kidneys, eyes and skin and send them to
- Global Hospital Mumbai,
- Care Hospital,
- Bombay Wockhardt,
- a Hospital from Pune,
- Mahatme Eye Hospital,
- OCHRI skin bank, etc.
ORGAN TRANSPLANT PROCESS
- Hospital Organ Donation registry coordinates the process of Cadaver Organ Donation.
- A transplant coordinator travels to the hospital to evaluate each potential donor & to determine the medical suitability of each organ. The transplant coordinator obtains detailed medical information about the patient’s current medical condition as well as any past medical history.
- The transplant coordinator meets with the potential donor’s next of kin, or other authorized party, to offer the opportunity of donation. This conversation is carefully timed and takes place only after the next of kin is given time to understand their loved one is brain dead.
- If the relative agrees to organ donation, he is asked to sign a consent form.
- The recovery of the organs is performed in operation theatre. The recovery team consists of surgeons, anaesthesiologists, nurses and the transplant coordinator.
- The organs are flushed with ice-cold preservative solution, packed in ice and placed in sterile containers to be transported to the recipient’s transplant centre. Heart & Lungs must be transplanted within 4 hrs after being removed from the donor. Livers – within 12 – 18 hrs, Pancreas – within 8 – 12 hrs, Intestines – 8 hrs & Kidneys – within 24 – 48 hrs.
- In such a scenario, a green corridor enables the healthcare facilities to transport vital organs from one place to another speedily. This requires an efficient coordinator between the hospital, the doctor’s team, the regional traffic authorities and awareness among masses.
Still, on a positive note, the donations are surely increasing day by day, and transplantation of kidney liver, pancreas, heart & lung are becoming more frequent because of technical developments & improvements in immunosuppression. However, the quality of donor management is a major determinant of the outcome of DBD donation. For improving the quality of donor care, one must have a fair knowledge of the patho-physiology of brain stem death.
Patho physiology of brain stem death
Brain death is often associated with marked physiological instability, which if not managed, can lead to a predictable pattern of complex multiple organ failure. Appropriate support before and after brain death can improve the number & quality of donor organs and hence skilled retrieval teams are important in the organization.(Table 1)
Neurological – Brain death is usually preceded by a variable period of raised ICP.
Cardiovascular – With increasing ICP, there is compensatory arterial hypertension, perhaps associated bradycardia, followed by marked sympathetic stimulation, with intense vasoconstriction, raised systemic vascular resistance, and tachycardia (a catecholamine storm). These are associated with central redistribution of blood volume, increased afterload, and visceral ischemia. The severity of changes depends on speed of onset of brain death. After the catecholamine storm, there is loss of sympathetic tone & peripheral vasodilatation. The resulting hypotension, if untreated, leads to hypo perfusion of all organs & may contribute to rapid donor loss.
Respiratory – Raised pulmonary hydrostatic pressure causes pulmonary oedema. If ventilation is not supported, resp. arrhythmia progresses to apnoea.
Endocrine, metabolic & Stress responses – After brain death, posterior pituitary function is very commonly lost, leading to diabetes insipidus with associated fluid & electrolyte changes. Thyroid hormonal changes may mimic “euthyroide sick syndrome” seen commonly in critically ill patients. Hyperglycaemia develops due to insulin resistance. Hypothalamic function is lost resulting in first hyperpyrexia followed by hypothermia.
An active inflammatory response occurs because of mediators released from damaged brain, ischemia – reperfusion injury, catecholamine storm and unstable cardiovascular state.
Coagulopathy is present in upto 34% of patients.
Table 1. Incidence of common physiological derangements in brain dead donors
| Derangement | Cause | Approximate incidence |
|---|---|---|
| Hypothermia | Hypothalamic damage, reduced metabolic rate, vasodilation and heat loss |
Invariable if not prevented |
| Hypotension | Vasoplegia; hypovalaemia; reduced coronary blood flow; myocardial dysfunction |
8114 – 97%25 |
| Diabetes insipidus | Posterior pituitary damage |
4525 – 78%35 |
| Disseminated intravascular coagulation |
Tissue factor release; coagulopathy |
2945 – 55%25 |
| Arrhythmias | ‘Catecholamine storm’; myocardial damage; reduced coronary blood flow |
2514 – 32%29 |
| Pulmonary Oedema | Acute blood volume diversion; capillary damage |
1325 – 18%14 |
The goals of organ donor management
Before the diagnosis of death, treatments are targeted to maximize the chances of patient survival rather than to support individual organs. After brain death, if donation is a possibility, an approach aimed at properly monitored balanced resuscitation of the donor & maintenance of all their organ systems ensures the greatest number of organs suitable for transplant.
In essence, donor management is a continuation of previous critical care management, but with a shift in goals. This mandates an effective CPR, invasive arterial monitoring, pulmonary artery catheterization etc.
Standardization of goals – Therapeutic goals and treatment guidelines have been formed based on expert opinion & current research. An institution can follow recommendation from organizations such as, The United Network for Organ Sharing (UNOS) or the Crystal City Consensus Conference Cardiac recommendations etc.
The Canadian multidisciplinary forum has recommended specific goals, which are included in the following table (Table 2)
Table 2. Suggested cardiovascular goals for the active management of potential organ donors
| Parameter | Target |
|---|---|
| Heart Rate | 60-120 beats min-1 |
| Arterial pressure | Systolic pressure >100 mmHg Mean pressure > 70 mmHg |
| Central venous pressure | 6-10 mmHg |
| Urine output | 0.5-3 ml kg -1h -1 |
| Electrolytes | |
| Blood Gases | Serum Sodium 130-150 mm of litre -1 Normal potassium, calcium, magnesium, phosphate Glucose4-8 mm of litre -1 |
| If pulmonary artery catheter inserted Pulmonary capillary wedge pressure |
pH -7.35 -7.45 paCO3 4.7-6 kPa paO2 > 10.7 kPa SPO2 saturation > 95% |
| Wedge pressure | 6-10 mmHg |
| Cardiac index | 2.4 litre min-1 |
| Systemic vascular resistance |
800-1200 dyn s cm-5 |
Practical aspects of Organ donor management
The principles of organ donor management are based on monitoring & therapies used in ICU and prompt change in therapy in presence of common derangements like hypothermia, hypotension and diabetes insipidus.
Temperature management – It includes active warming to maintain temperature > 350C before and during retrieval.
Cardiovascular support & fluid management – The first priority is to maintain an adequate, effective intravascular volume. There is no evidence that any specific fluid has particular advantages for resuscitation in donors. If crystalloids are given, balanced salt solutions may help avoid hyperchloremic acidosis. Blood & blood products should be used as per ICU protocol. High doses of starch-based colloids should be avoided in view of probable association with delayed graft function. The rate of IV infusion should be titrated according to the diabetes insipidus. Avoiding excessive fluid loading is associated with increase in number of transplantable lungs.
Cardiovascular function improves with use of catecholamines but higher doses of Dopamine and Norepinephrine (> 0.05µ Kg -1 min -1) in donors is associated with increased cardiac graft dysfunction.
Diabetes insipidus can be treated with low dose vasopressin, Canadian guidelines recommend vasopressin as the first choice vasopressor for donor resuscitation.
Some guidelines advocate thyroid hormone supplementation and is safe if overdose is avoided.
Ventilatory management – Lung damage from ventilator induced lung injury is common in ICU patients. So the strategy is now similar to the modern management of patients with acute lung injury (Tidal volumes of 6-8 ml Kg-1, PEEP, and measures to prevent derecruitment).
Management of Liver function – The liver suffers from acute haemodynamic changes at the time of brainstem death. The administration of methyl prednisolone reduces cytokine release both before retrieval & during surgery. It has been suggested that ischemic preconditioning of the liver in the heart beating donor might reduce IR injury. Volatile anaesthetic drugs and remifentanil have potentially beneficial preconditioning effects in hepatic & cardiac surgery, and could be investigated in organ donation.
Renal & Pancreatic function – Kidneys are vulnerable to catecholamine induced ischemia at the time of brain death, and subsequent hyperfusion if donor management is inadequate. Dopamine has no significant renal protective effect in critically ill patient and can be deleterious in donors if fluid management is inadequate.
Donor criteria for pancreatic graft retrieval are strict. Low vasopressor use and good glycaemic control are associated with increased numbers of retrieved grafts.
Inflammatory response and steroids – Methylprednisolone acts against the systemic inflammatory response associated with brain stem death if given in a dose of 15 mg Kg -1.
Table 3. Summary of the principles of donor management
Suggested approach
| General care 12-14 38 39 46-48 64 135 137 | Manage in ICU. Facilitates required nursing and medical care, and support for relatives. Minimum invasive cardiovascular monitoring includes arterial and central venous pressure. Cardiac output monitoring preferred. Review ICU therapeutic goals and alter to donor goals. Stop unnecessary drugs, e.g. sedatives. Reduce heat loss and actively warm if necessary to maintain care temperature > 350 C. Actively identify and treat any current infections. May require bronchoalveolar lavage (lung recruitment after. |
| Respiratory 7 38 72-76 | Use ‘lung protective’ ventilation. Tidal volume 6 – 8 ml kg-1 with optimal PEEP to allow minimum Fio2. Recruitment manoeuvres initially, and repeated after apnoea testing or tracheal suction. Maintain tracheal cuff pressure at 25 cm H2O and nurse with the head of the bed elevated to reduce the risk of aspiration. Avoid the administration of excessive i.v. fluids. Consider diuretics if marked fluid overload. |
| Cardiovascular 30-33 37-39 53 58 67 90 91 99 100 | Review fluid balance and correct hypovolaemia; be aware that vascular tone may be impaired. Use cardiac output monitoring if possible to titrate fluids and inotropic or pressor drugs to intended goals as guided by retrieval team. If vasopressor drugs required, vasopressin 0 – 2.4 units h -1* may reduce catecholamine requirements. High doses of catecholamine (e.g. norepinephrine > 0.05 |
| Fluids and nutrition 38 39 49 60 68 80 118-120 | |
| Blood and coagulation 38 43 44 55 60 138-140 | Correct coagulation if evidence of active bleeding; consider need for coagulation support during retrieval. Consider need for transfusion*. Maintain thromboprophylaxis as there is a high incidence of pulmonary emboli found at retrieval. |
| Systemic effects 15-17 35 39-42 108 | Methylprednisolone 15 mg kg -1 bolus immediately after brain death confirmed. Triiodothyronine*. |
| Investigations 29 30 50 58 67 75 | ECG, echocardiogram. Coronary angiogram may be indicated*. Bronchoscopy and lavage followed by lung recruitment manoeuvres. Chest X-ray after lung recruitment manoeuvres. |
Physiological support in the operating theatre
A multiple organ donation procedure involves midline laparotomy, extended by sternotomy, even if thoracic organs are not to be retrieved. There is potential for significant blood loss and hypothermia. Surgical manipulations cause cardiovascular instability, and vasoactive infusions are likely to be in progress. Maintaining stability during the procedure allows unhurried removal of organs in optimum undamaged condition. This can be demanding, and ideally donor support is provided by an appropriately experience individual from anaesthesia or critical care.
Spinal reflex movements are common and full neuromuscular block is required. Hypertension and increased plasma catecholamine concentrations have been observed during surgery and attributed to spinal reflexes. These can occur spontaneously or on surgical stimulus and have prompted some to suggest that anaesthesia for organ donors is required. However, marked spinal reflexes have been observed in the brain dead with liquefied cortex and cardiovascular changes are both generated and modifiable at spinal cord level alone. Hypertension may be moderated with vasodilators, opiates, or volatile anaesthetic agents. In addition, volatile anaesthetics may induce ischaemic preconditioning in hepatic and cardiac surgery. For this reason, some retrieval teams administer them during the last 30 min before aortic clamping.
What needs to be done more?
The successful implementation of cadaveric organ donation hinges on the education of masses & a more proactive attitude towards cadaveric organ donation. Proper counselling of relatives for organ donation in the event of brain death, proper hospital infrastructure, matching & distribution of the organs & coordination among hospitals play a major role.
The government needs to step in with resources to increase awareness from school days onwards. Chapters in schoolbooks & education while applying for voter card/driving licence could be introduced. Various awareness campaigns through media can be undertaken.
However, it is the need of hour that, regardless of a law on organ donation, people must come forth on their visit to be an organ donor after death. In addition, this can only happen if the govt. and healthcare facilities in an effective way. We should aim to follow the example of Croatia or Brazil. Croatia was able to increase their organ donation rate from 2.7 per million to 35 per million population over 10 yrs & today they are second in the world only to Spain. Recognizing organ donation as a priority area, earmarking requisite funds, sustained awareness campaign, training of transplant coordinators & appointing a key donation person in each hospital achieved this feat.
In India, millions are waiting for organs. Of those who are waiting, some have stepped forward to donate the healthy organs. They believe, they have more to give…!
So what’s stopping you? Pledge your organs today!
BE A GIVER……….. DONATE ORGANS!
References –
- Management of the heart beating brain dead organ donor – BJA 2012
- Cadaveric organ transplant – A new lease of Life – Aug. 2014 blogs – Fortis Healthcare.
- Cadaver organ donation & transplantation – An Indian Perspective – transplantation proceedings, org
- Manara AR, ct al, Donation after circulatory death – BJA 2012
- Barklin A. Systemic inflammation in the brain dead organ donor – act a Anesthesia Scand 2009
