
Anaesthesia for kidney Transplant
Anaesthesia for kidney Transplant- Kidney Transplants started way back in 2003 in Orange city Hospital,Nagpur.After initial hiccoughs & teething troubles,it started working smoothly & regularly.
Since then , 109 KT have taken place in OCHRI,including 16 cadaver or deceased donor transplants.
Deceased donor & Live donor KT , have differences in management of donor but management of the recepient is same.
In case of Live donor,patient is usually ASA I,without any major co morbidities,pre-evaluated & well prepared.
But,scenario is different with deceased donors,they are on high doses of multiple inotropes,electrolyte imbalances,polyurea,fluctuatin
In case of deceased donor,it’s important to manage donor till heart & liver are retrieved.as heart & liver retrieval take some time.To manage deceased donor till organ retrieval is a difficult task.
Anaesthesia for live kidney donor is same as any other GA with epidural,with special care towards hydration to maintain,kidney firm/turgid.Nephrectomy can be done laparoscopically or open. Postop pain is lesser in previous.
Anaesthesia for kidney recipient
It needs proper evaluation & preparation of patient for surgery as mostly patients are very much compromised, having problems of CRF,anaemia & poor veins.& need to optimise these patients to reduce postop complications,
Preoperative check.
1.Chronic anaemia.Hb around 8gm%
2.Due to recent hemodialysis,there is hypovolemia & residual anticoagulation.(usually patient is hemodialysed on pre-op day)
3.Post dialysis serum K level to be checked.
4.For IV,only one hand is available as another is having fistula.
Incidence of Hypertension is 90% & patient is usually on 3-4 antihypertensives .30% patients are diabetic too.
6 .IHD is common & usually silent ,especially in diabetics.
Incidence of calcified valvular heart disease is more’.
If dialysis is effective,pericardial effusion is rare.
7.Find out type of dialysis–Peritoneal or Hemodialysis.
If hemo–line or fistula.
8. Determine residual urine output per day.
9.Check for fluid overload( Pedal oedema/ basal crepts)
OR signs of Hypovolemia(postural hypotension,JVP,thirst,skin turgor,Urine output)
10.Allow 4-6 hrs elapse after hemodialysis before surgery to allow fluid equilibrium in body comparments & metabolism of residual heparin.
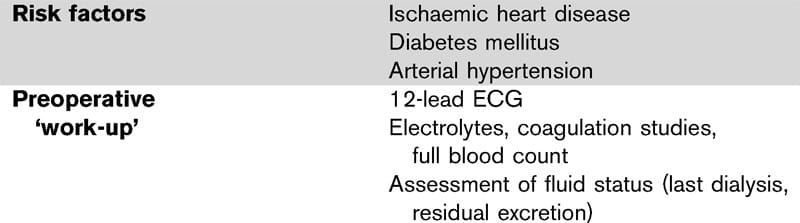 |
Investigations-—
1.CBC- Hb of 8 is acceptable as transfusion can precipatate hypertension & LVF.
2. LFT,KFT & Coagulation Profile–
Recent serum K is essential,if <6 mmol/L,dialysis will be required.
Hyponatremia can be found because of water retention.
Mild metabolic acidosis is frequent.
3.INR,APTT & Coagulation may be normal. uremia affects platelet function & can be improved by cryoprecipitate.
4.X-Ray chest ,ECG & Echo is important.
PERIOPERATIVE CARE–
1.Venous access & fistulae..Avoid IV line & BP cuff on arm with fistula.
2. Fluid load prior to induction– Wide swings in ABP are common.
3.These patients may have had multiple CVP lines,use ultra sound guidance for inserting CVP line.triple lumen central line is used.
4. These patients have low immunity,so strict asepsis should be followed.Methylprednisolone is given before graft is inserted.Patients receiving living donor kidney ,may profit from anti thymocyte globuline(given slowly over 60 min)
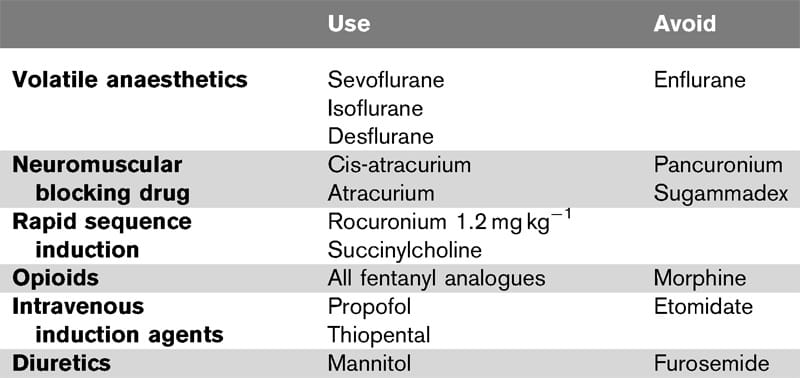
5.Suxamethonium is usually avoided.also avoid hypoventilation & hypercarbia.(to prevent hyperkalemia & acidosis)
careful correction of acidosis is recommended during surgery 1)bicarbonates, help to reduce hyperkalemia 2) function of transplanted kidney is supported.
6.Delayed Gastric emptying & increased acidity,make gastric reflux more likely.
7. Avoid K+ containing fluids,usually Normal saline or gelofusine is used.
blood loss should be replaced if at all there.
8.Commonly used agents are Isoflurane,Sevoflurane,Desflur
9.Prior to graft insertion ,slowly raise CVP to 10-12 mm of Hg,to maintain optimal graft perfusion & promote urine production.
Sometimes,Inotropes are required to increase blood pressure .Here,Noradrenaline is preferred. Dobutamine can be used for patients with low cardiac output,
10.Maintain Normothermia.Warm fluids should be administered as large amount of fluid is required.
continuous monitoring of electrolytes is required specially before & after reperfusion of transplanted organ.
11.once anastomosis is done ,fluid can be given freely ,chasing the output.
12 Patient.may be HBsAg & HCV positive,so staff should take due care.
 |
 |
POSTOPERATIVE.
.1.PCA morphine is suitable analgesic.
we are using IV paracetamol & contramol.
2.Epidural is possible,but there is danger of bleeding (secondary to abnormal platelets & effect of residual heparin if any) & problems with fluid loading & maintaining BP postoperatively.
3.Avoid NSAIDS & nephrotoxic drugs.
4.Maintain hypervolemia to promote diuresis.
5.continue Immunosupressants.
Proceedure— Transplantation of Cadaver or Live donor organ.
Time—–90 -180 min.
Pain ++/+++
Position –Supine
Blood loss–Not significant–about 500 ml.
Practical techniques—ETT,IPPV & CVP.
An extensive preoperative workup,to identify risk factors,to improve cardiac conditions,to treat hyperkalemia,& acid base balances along with optimal care of living donor,avoidance of nephrotoxic drugs,implementation of goal directed hemodynamic management & optimised postoperative care may improve outcome after renal transplant surgery.
Dr. Smita Harkare

