
Anaesthesiology: Rising Horizons
Introduction
Today we live in an environment where the safety and quality of anaesthesiology care has improved at least 10-fold over the past 20 years. Unfortunately, anaesthesiology still does contribute to major and avoidable complications and deaths and is still not completely safe for ASA I or II status patients. So, in order to achieve zero-defects in anaesthesiology-related harm, let’s see what new medications, devices, new technology and clinical decision support tools are on the horizon?
Future Anaesthesia Trends:
- Pre-operative testing will be performed in virtual clinics by a “cognitive assistant” type platform that will engage patients through interactive patient portals prior to procedural care. With analytical and reasoning capabilities, this automated routine work will support clinical decision-making.
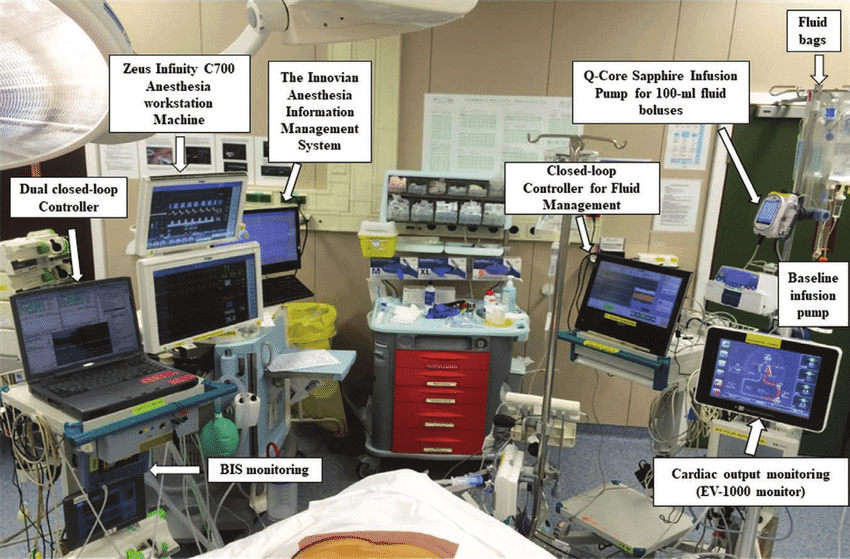
- Anaesthesia Information Management Systems (AIMS) with intraoperative monitoring device connectivity will provide decision support tools with real-time clinical guidance utilizing machine learning algorithms to predict things like hypotension long before it occurs clinically.
- Artificial Intelligence will transform patient care with
- Advanced Early Warning Systems (EWS) that utilize wireless surveillance to leverage algorithms for pattern recognition, allowing computers to detect slight variations in data with human-applied clinical rules (algorithms) that recognize patient deterioration and automatically activate interventions like rapid response teams, making “found dead in bed” a never event.
- Role of AI in Tele-anaesthesia: The concept of tele-anaesthesia could allow distant pre-operative assessment of the patient’s fitness for anaesthesia and also to regulate anaesthesia delivery in a far-off location with automated anaesthesia drug delivery systems maintaining a sufficient depth of anaesthesia.
Telemonitoring is one step ahead of telemedicine. The automated critical care system (ACCS) is under development in the United States. This system may be used to maintain intravenous anesthesia for a critically injured person during transportation from a remote location. - CLOSED loop automated drug delivery system (CLADS) – As the 21st century dawns, automated drug delivery has become increasingly prevalent.
The closed-loop anaesthesia delivery system (CLADS) is an indigenously developed patented (502/DEL/2003) computer-controlled anaesthesia delivery system. CLADS typically works with completed or “closed” feedback loop information elicited by BIS monitoring and delivers propofol TIVA to a patient via a non-TCI automated infusion pump. In one multicenter randomized controlled trial of CLADS using propofol and fentanyl, targeted to bispectral index (BIS) and heart rate, the CLADS maintained significantly tighter control than manual operation over BIS (P <0.0001) and heart rate within 25% of baseline (P <0.0031).
Automated anaesthetic systems incorporating independent closed-loops for hypnosis, analgesia, and fluid management are undergoing feasibility studies. - Robots for Anaesthesia
- Manual Robots include
-Kepler Intubation System (KIS) designed to utilise video laryngoscopy and a robotic arm to place an endotracheal tube with a claim of 91% success rate for oral intubation.
-DaVinci Surgical Robot to perform regional anaesthetic blockade.
– Magellan Robot designed to perform USG guided peripheral nerve blocks.
- Manual Robots include

- Pharmacological Robots
-Mcsleepy intravenous sedation machine, designed to administer propofol, narcotic and a muscle relaxant.
- I Control -RP machine closed loop system intravenous anaesthetic delivery system which makes its own decision regarding the delivery of Remifentanil and Propofol.
4. Monitoring inside the operating rooms: With innovation, monitoring has become less invasive like cardiac output monitoring or continuous noninvasive intra-arterial pressure monitoring by using blood pressure cuff applied to the finger such as CNAP system.Very soon cerebral pulse oximetry is going to unlock valuable data like brain autoregulation assessment.

Clinical information sometimes can be derived from established monitors via further in-depth analysis of the data already provided. The analgesia nociception index (ANI), surgical pleth index, and nociception level index (NOL) are examples using the nonlinear combination of heart rate, heart rate variability, photoplethysmograph wave amplitude, skin conductance, skin conductance fluctuations, and their time derivatives.

5. A New Novel Anaesthetic Agent will be available that combines the sedative-hypnotic drug properties of current medications with a rapidly titratable intravenous delivery system with a high therapeutic index and minimal side effects. This will go beyond small modifications of current medications like a proposed remimazolam and move us into a new generation of anaesthetics yet to be discovered.
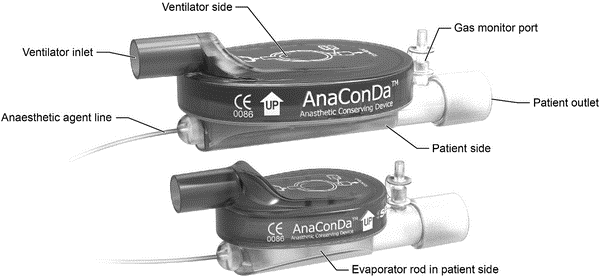
6.“AnaConDa” for delivering volatile anaesthetic in intensive and post-operative critical care: The anaesthetic conserving device, “AnaConDa” (Sedana Medical, Danderyd Sweden) is a simple, disposable, class IIa device that allows the inhaled anaesthetics isoflurane and sevoflurane to be safely and efficiently vaporized and delivered utilizing any non-rebreathing mechanical ventilator.
7.Role of Nanotechnology: Nanotechnology, coupled with AI, has the extraordinary capacity to monitor the human body at the molecular level. Nanotechnology is used in medicine for drug delivery, in vivo imaging, and nanotherapeutics. Nanoparticles, along with drug molecules, can target specific cells or tissues to delay drug metabolism and clearance and improve the drug’s bioavailability. In the coming days, it is possible to induce local anaesthesia by colloidal suspension containing millions of active analgesics instilled on the patient’s mucosa, and the nanorobots can guide these molecules deep into the tissue, even in the bone or teeth canal. In post-surgical pain, anesthetists may use new molecular targets, such as sodium channel blockers (Nav 1.3, Nav 1.7, and Nav 1.8); potassium channel openers in sensory neurons etc. Introducing nanocarriers inside the halothane molecule can increase its benefits as an anesthetic in the lungs and cardiovascular system and prevent liver exposure. Anaesthetic agents, such as Propofol, can improve anaesthesia quality using nanomedicine.
8.Role of Genomic Medicine: The concept of personalized medicine was introduced to overcome the inter-individual differences in the pharmacogenetics of a given drug. Pharmacogenomics exert a considerable influence on anaesthetic and surgical outcomes, thereby decreasing perioperative anaesthesia morbidity. Dexmedetomidine may produce variable vasoconstrictor response in individuals with a homozygous genetic variation at the AR-alpha-2BD allele. The subjects with mutations of NMDA (N-methyl-D-aspartate) and GABAA (Gamma-aminobutyric acid) receptors show the resistance to hypnotic effects of nitrous oxide or sedative and hypnotic effects of Propofol and etomidate. Gene expression in enhanced CYP2D6 activity may induce conversion of codeine to morphine resulting in a greater incidence of opioid-related side effects or vice versa. Genetic variations in the m-receptors are associated with exaggerated response of intrathecal fentanyl. Genetic variations in the hepatic enzyme CYP3A4 result in variable response to routinely-used drugs such as benzodiazepines, opioids, steroids, and 5HT3 antagonists.
The next 10 years will be challenging, no doubt, as we redesign healthcare delivery that personalizes patient-specific care, improves vigilance and patient safety through machine learning, virtual assistants and early warning surveillance systems. In this next decade, I am confident we will get closer to our goal of “ZERO HARM.”
BIBLIOGRAPHY
1. Anderson BJ, Bagshaw O: Practicalities of Total Intravenous Anesthesia and Target-controlled Infusion in Children. Anesthesiology. 2019;131(1):164–85. 10.1097/ALN.0000000000002657 [PubMed] [CrossRef] [Google Scholar] F1000 Recommendation
2. Hemmerling TM: Robots Will Perform Anesthesia in the Near Future. Anesthesiology. 2020;132(2):219–20. [PubMed] [Google Scholar] F1000 Recommendation
3. Aglio LS, Gugino LD, Mizuguchi KA: Commentary: At long last—Cerebral oximetry-based goal directed therapy to prevent postoperative cognitive decline is here. J Thorac Cardiovasc Surg. 2020;159(3):954–5. 10.1016/j.jtcvs.2019.03.066 [PubMed] [CrossRef] [Google Scholar] F1000 Recommendation
4. Tusman G, Bohm SH, Suarez-Sipmann F: Advanced Uses of Pulse Oximetry for Monitoring Mechanically Ventilated Patients. Anesth Analg. 2017;124(1):62–71. 10.1213/ANE.0000000000001283 [PubMed] [CrossRef] [Google Scholar] F1000 Recommendation 5. Purrucker JC, Renzland J, Uhlmann L, Bruckner T, Hacke W, Steiner T, Bösel J. Volatile sedation with sevoflurane in intensive care patients with acute stroke or subarachnoid haemorrhage using AnaConDa: an obervational study. Br J Anaesth. 2015;114(6):934–43. https://doi.org/10.1093/bja/aev070.
By Dr. Vrishali Ankalwar, Dr.Shweta Nayar
MD, DNB (Anesthesiology)
Dept. of Anesthesiology, GMCH ,Nagpur

