
Current status of regional anaesthesia techniques in cardiac surgery
DR VINAY KULKARNI
Consultant – Cardiac Anaesthesiology & Critical Care
VACCA, Nagpur
Optimal analgesia is an integral part of enhanced recovery after surgery (ERAS) programs worldwide which are designed to improve perioperative patient experiences and outcomes. Regional anaesthesia/analgesia provides a valid alternative for multimodal systemic analgesia.
Neuraxial blockade
Thoracic Epidural Anaesthesia (TEA) uses large 18G/16G needles for insertion of epidural catheter in the vascular epidural space. The catheter insertion should be done preferably a day before the surgery or atleast few hours before surgery to confirm normal neurological status n both lower limbs before surgery. TEA provides excellent quality of analgesia, can facilitate awake cardiac surgery and fast tracking of extubation in the operating room. However there is a definite, although low, risk of epidural hematoma formation ( 1:5493 to 1:12000 ) as reported in various series. Due to this potentially devastating complication in patients on full anticoagulation, its routine use is not recommended.
Intrathecal /Spinal Analgesia –can be administered using a small 27 G /25G needle and uses a single injection of the anaesthetic drug. Intrathecal morphine 5- 10 mcg/kg or clonidine can be used for providing effective perioperative analgesia after cardiac surgery, may help in reducing usage of systemic opioids. Intrathecal analgesia can reduce pain scores, reduce opioid usage, help in better preservation of pulmonary functions postoperatively.
Paravertebral blocks (PVB)
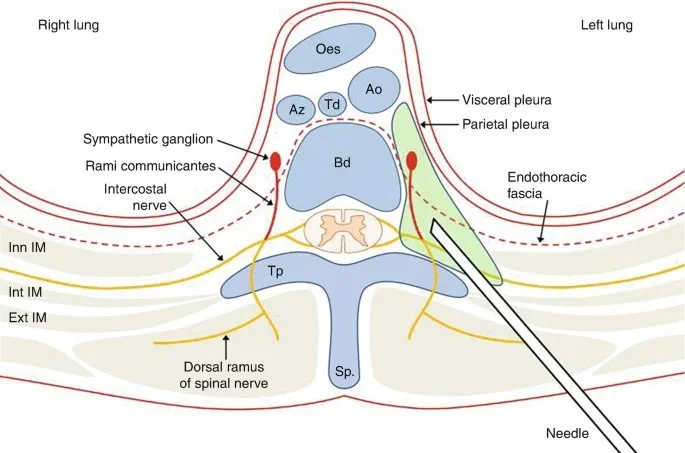
Unilateral PVB is used for thoracotomy, minimally invasive cardiac surgery, robotic surgery. Bilateral PVB can be used for midline /sternotomy pain, both either as single bolus or continuous infusion. Ultrasound guidance increases success rate. PVB can be considered for acute pain management following cardiac surgery.
Fascial Plane blocks
They are classified into posterior, lateral and anterior chest wall techniques, depending on the anatomical location. These are included as a part of the multimodal analgesic regimen for ERAS.
Posterior Chest wall Techniques
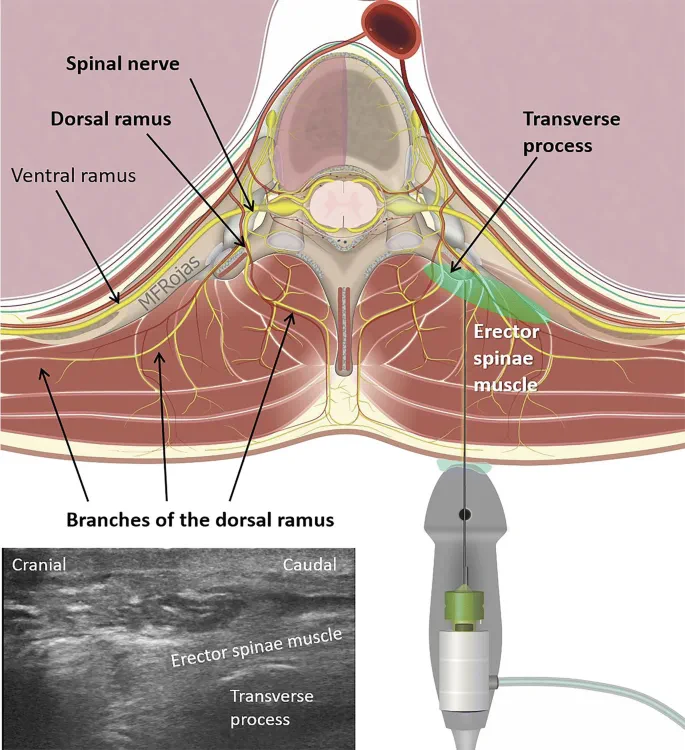
Erector Spinae Plane Block (EPSB) – This was initially described for chronic neuropathic pain, it s now being routinely applied for acute postoperative analgesia involving chest, thoracic, cardiac and abdominal surgeries.It can effectively block the dorsal and ventral rami of spinal nerves, when injected deep to the erecetor spinae muscle, at the level of T 6 transverse process. A single injection can result in effective spread in the craniocaudal plane. This is a relatively safe block, with a few theoretical risks.
Lateral Chest Wall techniques
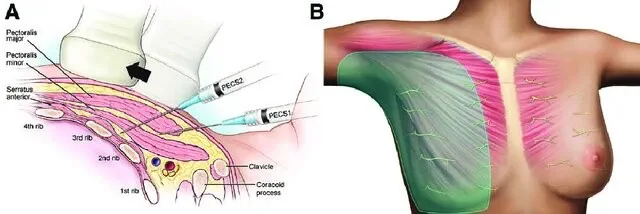
Pectoralis Major/Minor Block – An ultrasound guided pectointercostal fascial block (PIF) was introduced to provide analgesia to anterior chest wall innervated by anterior cutaneous branches of intercostals nerves, with an injection 2 cm lateral to the sternum between pectoralis major and internal intercostal muscles. Another injection between pectoralis minor and serratus anterior covers anterior chest, lateral wall upto axilla.
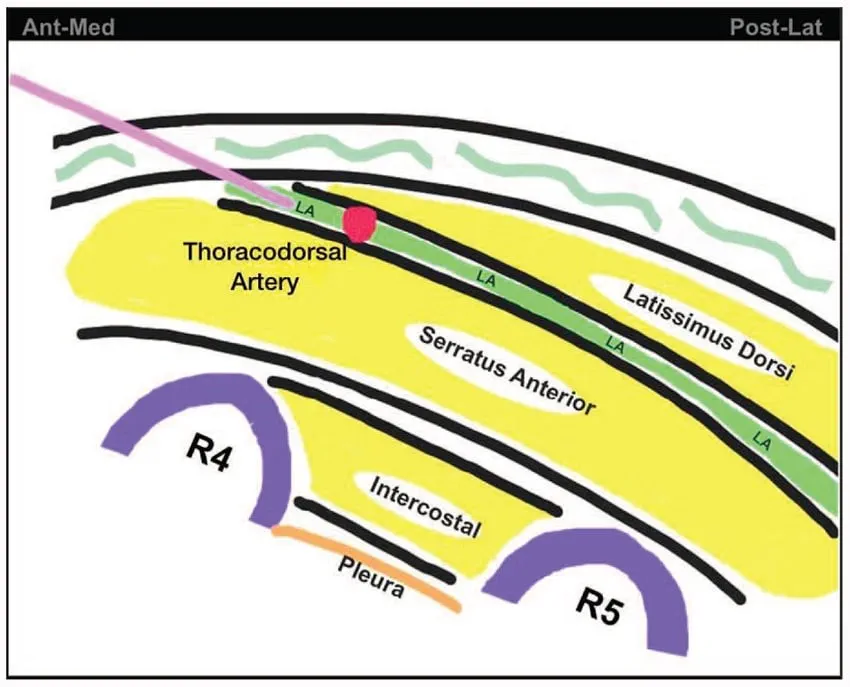
Serratus anterior Plane Block was devised primarily to block the thoracic intercostals nerves and provide analgesia to lateral thorax. In the midaxillary line, at the level of the 4th -5th ribs, local anaesthetic solution is deposited either anterior or deeper to the serratus anterior, under ultrasound guidance. This usually needs about 40 ml volume in adults.
Anterior Chest wall technique
Parasternal blocks target the anterior cutaneous nerve branchesof the intercostal nerves that innervate the anterolateral chest wall. They are divided into deep parasternal or transverses thoracic plane block ( TTPB) and superficial parasternal block or pectointercostal fascial block.
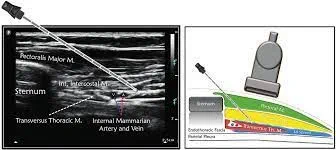
Due to recent emergence of these blocks, reports describing potential complications are scarce. Knowledge and skills in regional anaesthesia have become important for the cardiothoracic anaesthesiologist in today’s era of minimally invasive surgery and strive towards faster functional recovery and discharge. These blocks can provide superior analgesia and reduce opioid consumption after cardiac surgery.
Suggested reading
Regional anaesthesia in cardiac surgery: an overview of fascial plane chest wall blocks. Marta Kelava et al, Anesthesia and Analgesia July 2020, volume 131, number 1, 127-135

