
Older Airway Gadgets : Historical Perspective Of Airway Management Equipment
Dr Ketaki Marodkar
Professor,
Department of Anaesthesiology,
NKPSIMS & RC and Lata Mangeshkar Hospital, Digdoh,
Nagpur

“The point of human evolution is adapting to circumstance. Not letting go of the old, but adapting to the change is necessary!”
Airway gadgets play a pivotal role in anaesthesia as well as in cardiopulmonary resuscitation. Over centuries, these airway equipments have evolved dramatically to suit the requirements and to match the skill quotients of anaesthesiologists all over the world.
This write-up summarises few of such historical airway gadgets based on chronological order of development.
1827- Leroy’s intubation aid (Figure: 01) This endotracheal-tube introducer invented by urologist was withdrawn subsequently, for reasons unknown.

1829- The Babington’s glottiscope (Figure: 02) introduced, had a tongue depressor at one end and a mirror on the other. It was extremely complicated in design and bulky and was soon withdrawn.
1854– Manuel Garcia invented an indirect laryngoscope (Figure: 03): it hadjust a couple of mirrors, one of which deflected sunlight toward another one above the glottis. Its complicated design led to withdrawal.

1885- Joseph O’Dwyer’s airway (Figure: 04), resembled a modern supraglottic airway, except the variable-size tip was meant to sit in the glottis.

O’Dwyer’s intubation set (Figure: 05) was a pediatric kit that featured metal cylinders and blind introducers. The “blind” part demanded tactile skills and a willingness to use one’s fingers as bite blocks.

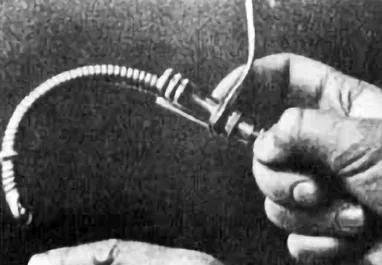
Kuhn endotracheal tube (Figure: 06) developed byHans Kuhn by developing a flexible metal tube with its own introducer. It had several metal rings leading to soft tissue trauma which led to withdrawal.
1895– Finally, a way to visualize the cords was found by Alfred Kirstein in 1895 as he invented an autoscope (Figure: 07) which could visualize patient’s trachea when placed in mouth.

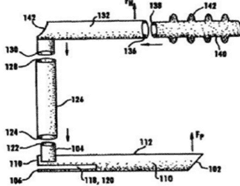
1902– German surgeon Franz Kuhn designed metal tubes that could be inserted through the mouth ‘blindly’ and also described the use of a curved tube introducer (Figure: 08), as well as being the first to publish a paper on nasal tubes (Figure: 09) and nasal intubation.


1920- 1980- This was the time when Sir Ivan Whiteside Magill developed endotracheal tube (Figure: 10). Magill and his assistant cut the tubes used for research from a roll of rubber tubing. The tubing inherited the memory of the cylindrical roll and Magill relied on this natural curvature to avoid the use of metal stylet. This is still referred to as the “Magill Curve”

He also developed twin-bladed tong-like Magill’s forceps (Figure: 11) to aid in lifting and guiding the nasotracheal tube into the larynx.

Magill’s laryngoscope blade (Figure: 12) was a straight-blade, with a U-shaped step and flange concave to the right which continued to be within an inch of the end of the blade.

The first metallic oral airway adjunct, was introduced in 1908 by anesthesiologist Frederic Hewitt (Figure 13).

Hewitt’s invention led to development of curved, plastic, disposable airways – the Guedel unit in 1933 and the Berman model with side channels in 1952.
1920-The early 1900s saw major advancements in laryngoscopy too, beginning with Chevalier Jackson’s laryngoscope (Figure: 14).

Later came Miller and MacIntosh—who introduced straight and curved blades in 1941 and ’43, respectively. MacIntosh felt that
his model was superior because it had less contact with the epiglottis, but choosing between the two remains a matter of personal preference for the rest of us(Figure:15).

1937– The first supraglottic airway was Beverly Leech’s Pharyngeal Bulb Gasway (Figure 16). Mostly metal and relatively inflexible, Leech’s “bulb” was the inspiration for modern inflatable plastic seals.

1968- The first Supraglottic airway device carried by pre-hospital caregivers was the esophageal obturator airway (Figure 17).

Thus we see the mesmerizing historical airway gadgets and these were artistically modified to achieve a safer airway handling nowadays.

