
Expanding Horizons: Labour Analgesia – A Road Towards Standard Obstetric Care
Dr. Heena D. Pahuja
Professor, Dept. of Anesthesiology
NKPSIMS & LMH, Nagpur

Labour analgesia refers to the use of various methods to alleviate pain during childbirth while ensuring maternal and fetal safety.
The experience of delivering a baby into the arms of a conscious, pain-free mother is considered as one of the most fulfilling moments in medicine, as highlighted by Moir. However, achieving effective pain relief during labour has long been surrounded by myths and controversies, presenting on-going challenges. The foundations of obstetric anaesthesia were laid by James Young Simpson, who introduced ether for pain relief during childbirth in a woman with a deformed pelvis. Despite its ground breaking nature, his approach, termed “etherisation of labour,” faced harsh criticism and moral opposition. This debate persisted until 1853 when John Snow famously administered chloroform to Queen Victoria during the birth of Prince Leopold, her eighth child, marking a turning point in societal acceptance of labour analgesia.
In modern obstetric practice, neuraxial labour analgesia represents a significant shift, emphasizing not only pain relief but also the overall quality of analgesia provided to mothers. This evolution aligns with broader efforts to address women’s pain comprehensively. The International Association for the Study of Pain (IASP) dedicated 2007-2008 as the “Global Year against Pain in Women – Real Women, Real Pain,” focusing on both acute and chronic pain in women to improve care and outcomes.
Role of obstetric anaesthesiologist for providing pain relief during labour has emerged as the subspecialty with the use of modern anaesthetic technique.
Pain Pathway in Labour
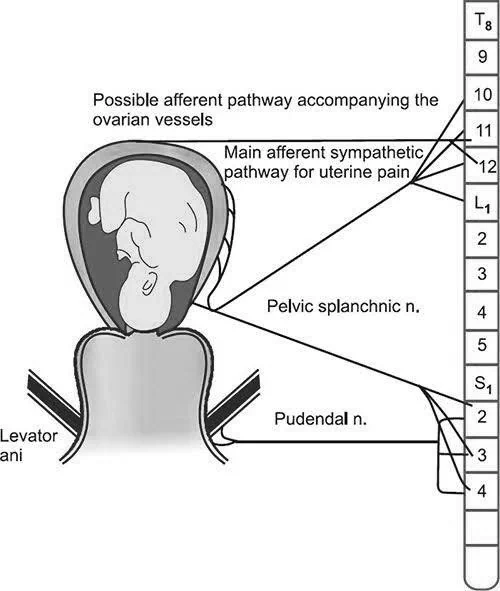
The pain in labour is primarily visceral, originating from the uterus and cervix, transmitted via the pelvic nerves (T10-L1) and the pudendal nerve (S2-S4). These signals travel to the brain, where they are processed as pain. Analgesia aims to interrupt these pathways at various levels to reduce pain perception. The pain score during labour according to McGill Pain Questionnaire is almost similar to that of digit amputation.
Types of Labour Analgesia
A] PHARMACOLOGIC ANALGESIA: Requires active involvement of an anaesthesiologist.
1) Systemic analgesia: Includes parenteral drugs (opioids like morphine, fentanyl) and inhalational agents.
a) Intravenous (IV) Opioids: such as morphine or fentanyl or remifentanyl may be used for pain relief, though they do not provide complete analgesia and can have side effects such as sedation and nausea.
b) Low dose ketamine analgesia– In 1st stage of labour bolus dose of ketamine 10-15 mg followed by infusion of 0.5-1 mcg/kg/min is given. At the time of crowning 0.2-0.4 mg/kg can be repeated. Dose should not exceed 100 mg.
METHOD OF ADMINISTRATION
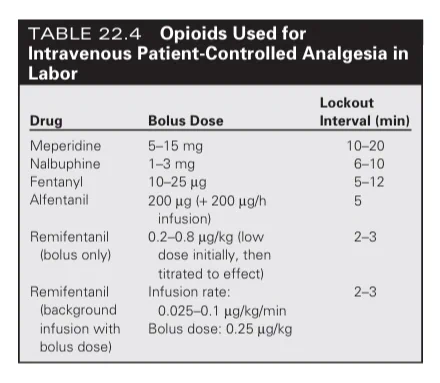
Intravenous Patient-controlled analgesia: The parturient can tailor the administration of analgesia according to her individual needs by using PCA pumps.
| OPIOIDS USED FOR INTRAVENOUS PATIENT CONTROLLED ANALGESIA IN LABOUR |
c] Inhalational agents
- Nitrous Oxide (Entonox): N2O is blended with O2 in 50:50 ratio, this provides mild pain relief, commonly used in early labour.
- Volatile Halogenated Agents: All volatile halogenated agents like enflurane, desflurane, isoflurane, sevoflurane provide analgesia and also cause dose-dependent relaxation of uterine smooth muscle.
2] Neuraxial analgesia Epidural and spinal anaesthesia are the most effective options. Epidurals provide continuous pain relief via a catheter in the epidural space, while spinal anaesthesia offers quick, profound relief through a single injection into the subarachnoid space. In this type of analgesia, role of an anaesthesiologist is indispensible.
a) Epidural Analgesia- is the most commonly used technique for pain relief during labour. It involves the continuous infusion of a local anaesthetic (e.g., bupivacaine) with or without opioids (e.g., fentanyl) into the epidural space through a catheter. Provides continuous pain relief, allowing for adjustments in medication throughout labour. It is effective for both early and late stages of labour and can be used for both vaginal deliveries and cesarean sections. It can also be used for operative procedures if required.
Current ASA guidelines suggest that maternal request for labour pain relief is sufficient justification for epidural initiation and the timing should not depend on an arbitrary cervical dilation.
b) Spinal Analgesia: involves a single injection or as a continuous infusion of opioids with or without small dose of local anaesthetic into the subarachnoid space. It provides rapid, profound analgesia and is typically used when fast pain relief is required, preferably in 2nd stage of labour.
c) Combined Spinal-Epidural (CSE) Analgesia – A small dose of local anaesthetic and opioids is injected into the subarachnoid space, providing rapid pain relief, while an epidural catheter is used for continuous analgesia throughout labour. This technique offers the advantage of quick onset with the flexibility of long-term pain control if needed.
Ambulatory / Walking Neuraxial Analgesia: The term “walking” or “mobile” epidural analgesia was first coined to describe low-dose CSE opioid analgesia. Here motor function is maintained and the ability to walk is not impaired.
d) Dural Puncture Epidural: utilizing the “needle-through-needle” technique and the Dura is punctured by 25- or 26-gauge spinal needle, no medication is directly introduced into the intrathecal space but the Dural puncture may facilitate the intrathecal migration of medication administered into the epidural space. DPE has been associated with a decreased time to adequate analgesia after block placement.
METHOD OF ADMINISTRATION
Patient-controlled epidural analgesia (PCEA), or Programmed intermittent epidural bolus (PIEB): PCEA allows the patient to self-deliver a dose through the epidural catheter with the use of a pump that limits the maximum drug dose per hour to prevent toxicity, whereas PIEB utilizes a pump that gives automated boluses at a fast rate at set intervals instead of a slow continuous infusion.
| DRUGS USED FOR EPIDURAL & SPINAL ANALGESIA: |

3] OTHER REGIONAL NERVE BLOCKS: Various blocks like paracervical block, pudendal block, sacral block, caudal block and lumbar sympathetic block can be given for labour analgesia.
Use of ultrasound guidance for epidural and other regional blocks has improved success of labour analgesia in obese parturients.
B] NON PHARMACOLOGIC ANALGESIA: Techniques like
- Intradermal Water Injections
- Transcutaneous Electrical Nerve Stimulation
- Breathing exercises – Lamaze technique
- Massage
- Aromatherapy
- Hydrotherapy
- Therapeutic use of heat & cold
- Leboyer’s technique
- Acupressure/acupuncture
These are mainly given by trained Obstetrician. These can supplement pharmacologic methods but are less effective in severe pain.
Advantages of Labour Analgesia
- Provides effective pain relief, improving maternal comfort.
- Minimal fetal effects, especially with regional techniques.
- Facilitates obstetric interventions, such as caesarean sections.
- Reduces maternal stress and improves the birth experience.
Conclusion:
Advancements in the understanding of pain physiology, pharmacological interventions, and the evolution of obstetric anaesthesia as a specialized field have revolutionized labour pain management. The widespread adoption of regional analgesia as a standard of care highlights its importance in improving maternal satisfaction and clinical outcomes. Notably, modern research has debunked myths surrounding early neuraxial analgesia, demonstrating its safety and efficacy without compromising delivery outcomes. Emerging innovations, such as algorithm-driven PCEA systems and automated bolus delivery, promise to further enhance the precision and effectiveness of labour analgesia. As technology and research continue to evolve, the future of obstetric anaesthesia holds great potential to set new benchmarks in labour analgesia.
References:
- Gropper MA, Eriksson LI, Fleisher LA, Wiener-Kronish JP, Cohen NH, Leslie K, editors. Miller’s anaesthesia, 2-volume set E-book. Elsevier Health Sciences; 2019 Oct 7
- Chestnut DH, Wong CA, Tsen LC, Kee WD, Beilin Y, Mhyre J. Chestnut’s obstetric anaesthesia: principles and practice e-book. Elsevier Health Sciences; 2014 Feb 28.
- Healy TE, Knight PR, editors. Wylie Churchill-Davidson’s A Practice of Anesthesia 7th Edition. CRC press; 2003 Oct 31.
- Pandya ST. Labour analgesia: Recent advances. Indian journal of anaesthesia. 2010 Sep 1;54(5):400-8.
- Lam KK, Leung MK, Irwin MG. Labour analgesia: update and literature review. . 2020.

