
GERIATRIC ANAESTHESIA; A DISTINCT SUB SPECIALTY
Dr. Devayani Thakur
Consultant Anaesthesia and Pain management,
Medworld Hospital, Nagpur
Suretech Hospital, Nagpur

Introduction
Geriatric anesthesia is defined as a specialized anaesthesia care focused on elderly patients aged 65 years and older. With the increasing life expectancy and advanced healthcare facilities, increasing number of surgeries are performed on geriatric people.
Each elderly patient is unique with varying physiological capacities and comorbidities, a signature made plan of anaesthesia should be tailored to the needs of this subset of patients.
Physiologic changes of elderly:
- Cardiovascular system: Reduction in cardiac output and myocardial contractility, stiffer vessels, increased systemic vascular resistance, impaired baroreceptor sensitivity, leads to increased chances of intraoperative and post-operative hypotension, arrhythmias, MI and decreased tissue perfusion.
- Respiratory system: Decreased lung compliance due to stiff chest wall and decreased lung elasticity, decreased vital capacity and respiratory drive, VQ mismatch leading to postoperative respiratory complications.
- Renal: Nephrosclerosis resulting in decreased GFR and creatinine clearance along with altered ability to dilute and concentrate urine. Serum creatinine maybe normal due to decreased muscle mass.
- Hepatic: Decreased – liver volume, intrinsic metabolism, hepatic blood flow and slower drug metabolism.
CNS: Decreased cerebral blood flow, loss of neurons. This leads to increased neurotoxicity from anesthetic agents and predispose them to the increased risk of cognitive complications like postoperative cognitive disorders (POCD) and delirium.
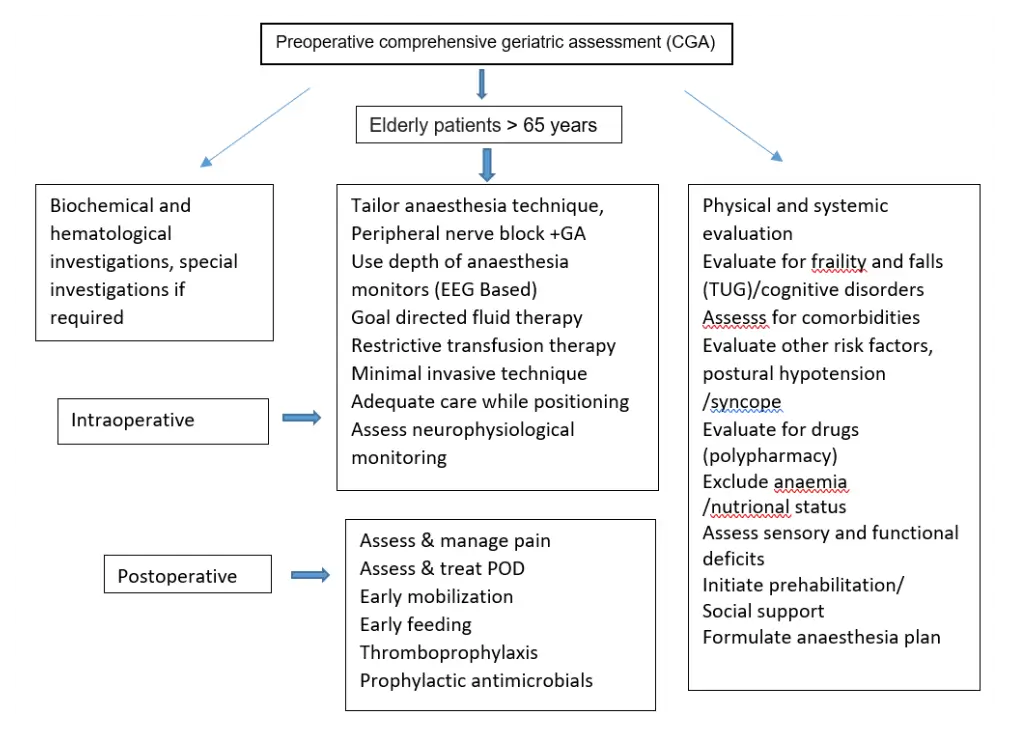
Preoperative assessment:
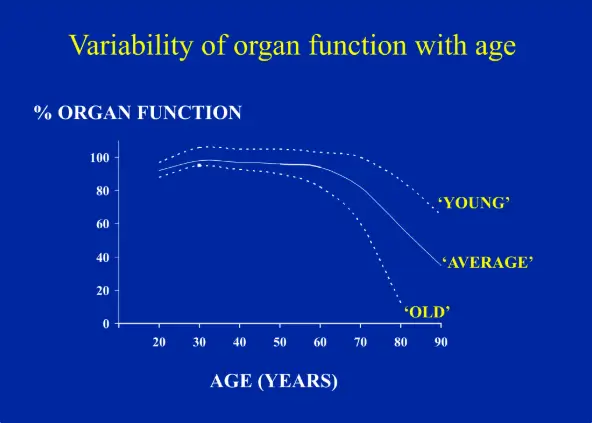
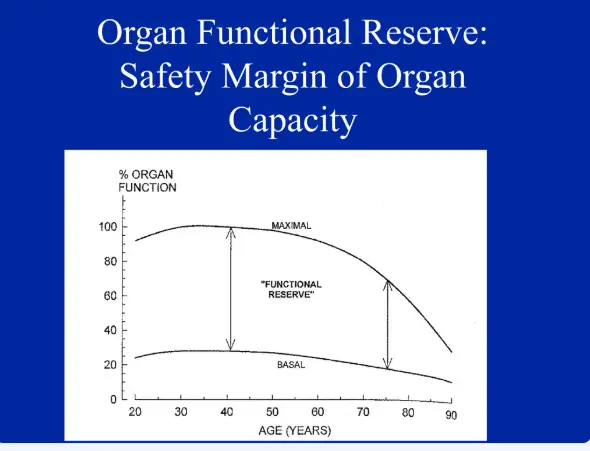
It should focus on patient’s history, physical examination, diagnostic studies, determination of functional capacities, functional physiologic reserves along with the comorbidities. Assessment of the frailty index and Clinical frailty scale which refers to the state of reduced physiological reserve and increased vulnerability to stress and categorizes patients from very fit to severely frail respectively.
A comprehensive evaluation of cognitive function should also be evaluated by screening tools like Mini Mental State Examination (MMSE), Montreal cognitive assessment (MoCA). Nutritional status should also be evaluated by Mini nutritional assessment (MNA).
Incorporating these assessments may help in prehabilitation before the surgery to improve the resilience and postoperative outcomes and to reduce the complications, shorten the hospital stay and better functional recovery.
Choice of Anaesthesia :
Regional versus general Anaesthesia
There is a growing evidence that regional anesthesia may be preferred over general anesthesia in elderly patients to avoid systemic effects of drugs. However, regional anesthesia may possess its challenges in the elderly like: anatomical changes in spine, kyphoscoliosis, use of anticoagulants. Hence the decision to use regional anesthesia should be individualized based on patient’s profile.
Regional anaesthesia is also recommended in ERAS protocols to decrease the poly pharmacy, need for opioids, postoperative pain and the risk of POCD.
Poly pharmacy and drug interactions:
Polypharmacy is defined as use of more than five drugs at the same time. Most geriatric patients are usually on multiple drugs, which can cause drug interactions and adverse reactions hence pre-operative assessment to identify them and dose adjustment is essential.
The choice of anaesthesia can be based on following points:
- General anaesthesia: Reduced drug doses, use of short acting agents, careful intraoperative and postoperative monitoring with neurological monitoring (BIS) must be considered.
- Regional Anaesthesia: Offers advantages but requires expertise due to anatomical changes of old age and concomitant use of antiplatelet/ anticoagulants, doze adjustment due to change in volume of distribution.
- Local Anaesthesia: Preferable for minor procedures to avoid risks of general anaesthesia.
Balanced Anaesthesia using combination of agents and methods, minimize the risk while achieving effective anesthesia and early recovery.
Intra Operative monitoring:
- Hemodynamic monitoring: continous NIBP, HR, SPO2, ETCO2 should be monitored along with neurological monitoring wherever possible.
- Ventilatory support: tailored ventilation strategies should be considered due to various respiratory changes.
- Fluid management: meticulous fluid balance is maintained due to reduced renal, cardiac functioning and potential fluid overload.
- Careful positioning of these patients with proper padding.
- Temperature regulation: geriatric patients are at high risk of hypothermia, so active warming measures should be considered.
- Pain relief, assessed by NRS, verbal rating scale or pain in advanced Dementia and Doloplus-2 scales (PAINAD), should be given by multimodal analgesia and minimized use of opioids.
Post-operative Complications:
a) Postoperative POCD and delirium, hyponatremia, increased hospital stay.
b) Cardiorespiratory complications like: MI, arrhythmias, cardiac failure, circulatory failure, fluid imbalances, respiratory failure, atelectasis, pneumonia.
c) DVT, bed sores: early mobilization to prevent these complications and to speed up the recovery.
Multidisciplinary approach:
A team approach should be given towards geriatric patients by a collaboration between anesthesiologists, surgeons, geriatricians, nurses, nutritionists and physical therapists.
Challenges of geriatric anesthesia:
- Due to physiologic changes and comorbidities of geriatric patients and the increased risk of complications.
- Lack of consensus on standardized guidelines for anaesthesia practices in elderly.
- Anesthesiologists and the collaborative team must be trained to recognize and manage geriatric issues.
Future for geriatric Anaesthesia:
- There is a need for further research and evidence based guidelines to define best practices for elderly anaesthesia care.
- A need for focused anaesthesia training programs and education.
- With the advancements in AI, advanced monitoring techniques should be used to predict the complications in real time.
Geriatric anesthesia is thus a distinct sub speciality requiring a tailored approach to address the unique anatomical, physiological and pharmacological challenges of aging.
Hence the field of geriatric anesthesia has to be given significant importance to provide sound and effective healthcare and better outcomes.
References:
- Recent advances in geriatric anaesthesia
Mahender, Anuradha; Chavan, Surekha S.1; Saroa, Richa2; Chauhan, Meenal3
Author Information: Indian Journal of Anaesthesia 67(1): p 152-158, January 2023. | DOI: 10.4103/ija.ija_1029_22 - Anaesthesia in the Elderly
Dr Nigel Hollister, registrar ICU, Christchurch hospital, New Zealand
Email: nigel.hollister@doctors.org.uk
20th May 2006 - Anesthetic management of geriatric patients
Korean Journal of Anesthesiology 2020; 73(1):8-29.
Published online: October 22, 2019
DOI: https://doi.org/10.4097/kja.19391 - Recent advances in geriatric anaesthesia
Anuradha Mahender 1,✉, Surekha S Chavan 1, Richa Saroa 2, Meenal Chauhan 3 Indian J Anaesth. 2023 Jan 21; 67(1):152–158. doi: 10.4103/ija.ija_1029_22 - Perioperative care of the elderly
David Murray, Chris Dodds
Continuing Education in Anaesthesia Critical Care & Pain, Volume 4, Issue 6, December 2004, Pages 193–196, https://doi.org/10.1093/bjaceaccp/mkh052 - Published: 01 December 2004
Miller’s Textbook of Anaesthesia: Geriatric Anaesthesia
Fredrick Siber, Ronald Pauldine Pages 2407-2422

